Ctq to aces preprint 20221107 - Tài liệu tham khảo | Đại học Hoa Sen
Ctq to aces preprint 20221107 - Tài liệu tham khảo | Đại học Hoa Sen và thông tin bổ ích giúp sinh viên tham khảo, ôn luyện và phục vụ nhu cầu học tập của mình cụ thể là có định hướng, ôn tập, nắm vững kiến thức môn học và làm bài tốt trong những bài kiểm tra, bài tiểu luận, bài tập kết thúc học phần, từ đó học tập tốt và có kết quả
Môn: Social Phsycology (PSYC 241) 53 tài liệu
Trường: Trường Đại học Hoa Sen 5.3 K tài liệu
Tác giả:














Preview text:
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
Running head: ADVERSITY QUESTIONNAIRE CORRESPONDENCE
Correspondence between the Childhood Trauma Questionnaire
and Adverse Childhood Experiences questionnaire Theresa W. Cheng ,
1,2 Martin H. Teicher , Kristen Mackiewicz 3 -Seghete4 1 2
Masschusetts General Hospital, University of Oregon,
3McLean Hospital and Harvard Medical School,
4Oregon Health & Sciences University Author Note
Theresa W. Cheng, Psychiatric & Neurodevelopmental Genetics Unit, Massachusetts
General Hospital and Dept. of Psychology, University of Oregon., Martin H. Teicher,
Developmental Biopsychiatry Research Program, McLean Hospital, and Dept. of Psychiatry,
Harvard Medical School, Kristen Mackiewicz-Seghete, Dept. of Behavioral Neuroscience,
Oregon Health & Sciences University.
Correspondence concerning this article should be addressed to Theresa W. Cheng,
Psychiatric and Neurodevelopmental Genetics Unit, Simches Research Building, 185 Cambridge
Street, Boston, MA 02114, Email: t wcheng@mgh.harvard.edu .
Author TWC was supported by the National Center for Advancing Translational Sciences
of the National Institutes of Health under award number TL1TR002371 and by the National
Institute of Mental Health under award number 1F31MH124353-01. The content is solely the
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
responsibility of the authors and does not necessarily represent the official views of the National
Institutes of Health. The authors declare no competing financial interests.
ADVERSITY QUESTIONNAIRE CORRESPONDENCE Abstract
Childhood adversity is commonly measured via retrospective self-report on the Adverse
Childhood Experiences (ACE) questionnaire and the Childhood Trauma Questionnaire (CTQ).
To facilitate comparison of studies and data employing these measures, we employed a variety of
approaches to equate CTQ and ACE questionnaire responses pertaining to emotional, physical,
and sexual abuse, as well as emotional and physical neglect. The accuracy, sensitivity, and
specificity of these approaches suggest moderate to strong levels of questionnaire
correspondence in a sample of middle-class young adults living in the United States (N=471; 273
female; mean age=23 years, SD=1.7 years) across maltreatment types, except for physical
neglect (which exhibited poorer and more variable correspondence across approaches). Results
in a validation sample (N=64; 43 female; mean age=19.1, SD=0.5) did not suggest model
overfitting. We also provide an interactive web-based tool to examine questionnaire
correspondence across approaches.
Keywords: childhood adversity, childhood maltreatment, adverse childhood experiences,
Childhood Trauma Questionnaire, measurement
ADVERSITY QUESTIONNAIRE CORRESPONDENCE Introduction
Childhood adversity is a significant risk factor for physical and mental health problems
(e.g., Felitti et al., 1998; Gilbert et al., 2015). While diverse measures are used to assess
exposures to such adversities, their comparability is rarely considered. Two of the most used
retrospective self-report measures of childhood adversity are the Adverse Childhood Experiences
(ACE) questionnaire and the Childhood Trauma Questionnaire (CTQ) (Norman et al., 2012).
This report aims to provide a quantitative basis for understanding the comparability of these
questionnaires, specifically regarding the way they measure maltreatment. Addressing this may
help resolve inconsistencies in the literature and shed insight into when it may be appropriate to
collapse across samples using different measures in secondary data analyses.
These questionnaires were each developed for distinct purposes within different
disciplinary traditions. Early on, the ACE questionnaire was administered via mail-in surveys to
study the impacts of childhood adversity on mortality risks (Felitti et al., 1998). ACE screening
has been adopted in healthcare settings (Koita et al., 2018) and proposed in policy (e.g., ACEs
Aware initiative; www.acesaware.org), though some caution against this (Finkelhor, 2018). The
ACE questionnaire commonly assesses five types of childhood maltreatment (emotional,
physical, and sexual abuse; emotional and physical neglect) and experiences characterized as
household dysfunction (e.g., witnessing domestic violence or the incarceration of a caregiver),
though versions vary. The questionnaire is not psychometrically ideal in its use of single binary
items for each exposure. However, its brevity facilitates ease of administration, and typical uses
emphasize cumulative risk rather than an accurate assessment of single experiences (although
researchers do examine associations with specific items, e.g., Norman et al., 2012).
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
Researchers and mental health professionals developed the CTQ to assess the same five
aforementioned types of maltreatment. It was developed with a sample of adolescent psychiatric
inpatients (Bernstein et al., 1997) and refined into a brief version (Bernstein et al., 2003). Its
psychometric properties have been examined in clinical and community samples worldwide
(Klinitzke et al., 2012; Grassi-Oliveira et al., 2014; Kim et al., 2011; Gerdner & Allgunlander,
2009). Compared to the ACE questionnaire, the CTQ is longer, more detailed, and expressly
assesses the frequency of occurrence; due to this greater detail, research ethics committees may
less commonly approve its use, especially for studies with sensitive populations.
This brief methodological report aimed to evaluate the correspondence of the ACE
questionnaire and CTQ in a sample of middle-class young adults living in the United States.
Across five types of maltreatment, we used a variety of approaches to transform richer, multi-
item Likert-scale CTQ data into binary scores. We then calculated metrics comparing these
scores to binary ACE questionnaire responses, including accuracy, sensitivity, specificity, and
area under the curve in receiver operating characteristic (ROC) plots. Methods
Participants and Procedures
We fit models within a discovery (aka training) sample using exploratory procedures to
identify optimal parameters. Our discovery sample of 471 subjects (273 female) ages 20-27 years
(M=23, SD=1.7) was obtained with permission from the authors of a prior instrument validation
study (Teicher & Parigger, 2015). Participants were recruited from the community via
advertisement and were medically healthy, right-handed, unmedicated, with no history of
significant head trauma. After an initial phone screening, participants completed surveys online
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
via a HIPAA-compliant system, which included the ACE questionnaire. Based on these scores,
invitations to the full session ensured equal representation of those exposed to zero, one, two,
three, and four or more types of maltreatment. In the full session, participants completed surveys,
clinical assessments, and underwent neuroimaging. For full details on procedures used with
participants in the discovery sample, see Teicher and Parriger (2015).
We also used a validation (aka test or hold-out) sample to inform study generalizability.
The validation sample of 64 subjects (43 female) was from a study that recruited medically
healthy 18–19-year-old participants (M=19.1, SD=0.5; one enrolled at age 19 but completed the
study at age 20) with scores of either 0 or greater than 2 on a different adversity questionnaire
(Maltreatment and Abuse Chronology of Exposure; Teicher & Parriger, 2015). Participants in the
validation sample were enrolled, interviewed, and assessed similarly.
All participants provided written informed consent before participation. Studies were
approved by the [removed for blind review], with continuing review through [removed for blind
review], which subsumed the [removed for blind review]. See Table 1 for a summary of
sociodemographic variables and adversity prevalence across samples. Measures
Adverse Childhood Experiences (ACE)
The ACE questionnaire included ten binary (yes/no) self-report items, each regarding a
type of adverse childhood experience (Felitti et al., 1998). The five items pertinent to this report
assessed emotional, physical, and sexual abuse, as well as emotional and physical neglect.
Childhood Trauma Questionnaire (CTQ)
This measure assessed the same five types of maltreatment with five items each; for each
item, individuals responded using a five-point scale regarding the frequency of exposure (from
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
“Never True” to “Very Often True”; Bernstein et al., 1997). Three items addressed minimization
or denial. See Supplementary Table 1 for a comparison of the CTQ and ACE questionnaire. Data Analysis Missing Data
On the ACE questionnaire, 13 participants were missing data (number of missing items:
emotional abuse=2, physical abuse=7, sexual abuse=2, emotional neglect=1, physical neglect=1).
As the ACE items were modeled as outcome variables, data were excluded for analyses within
maltreatment type. On the CTQ, 13 participants were missing data, each on a single item
(emotional abuse=1, physical abuse=2, sexual abuse=2, emotional neglect=4, physical neglect=4;
minimization=0). Values were mean-imputed within maltreatment type.
Transforming CTQ values
Continuous CTQ responses were transformed into binary scores (referred to as “predicted
ACE scores”) and compared to binary ACE responses for each maltreatment type. As there is no
existing standard transformation, we explored several transformations.
Item-based Thresholds. On the ACE questionnaire, participants were instructed to
endorse an item if any of a list of experiences occurred to them at a specified frequency before
18 years of age. On the CTQ, participants indicated the frequency of exposure to experiences in
separate items. Here we conceptualized the CTQ as breaking apart a single compound ACE item
into components (although their wording differs, see Supplementary Table 1). If a participant
endorsed one or more relevant CTQ items at a frequency at or higher than the frequency
specified on the ACE questionnaire (“ever” for sexual abuse, interpreted as a frequency response
of “rarely” on the CTQ; “often” for all other types of maltreatment) their predicted ACE score
was “yes.” Otherwise, it was “no.”
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
Subscale-Based Thresholds. This approach applied thresholds to summed CTQ items.
We examined algorithmically-generated thresholds (using OptimalCutpoints v 1.1-4 in R ), first
identifying thresholds that maximized sensitivity and specificity via Youden’s index (Youden,
1950; emotional abuse=9, physical abuse=7, sexual abuse=6, emotional neglect=12, physical
neglect=8). As is typical for low-prevalence outcomes, this resulted in a high false positive rate
(Bernstein et al., 1997). In a second approach, we identified thresholds using a fixed costs ratio
of 0.5 (McNeil et al., 1975; Smits, 2010; emotional abuse=11, physical abuse=8, sexual abuse=7,
emotional neglect=14, physical neglect=14), such that false positives and false negatives were
considered equally “costly”. The number of misclassified individuals was reduced overall.
Machine learning. A support vector machine is a common supervised machine-learning
approach to binary classification (Cortes & Vapnik, 1995). This method identified a hyperplane
in a multi-dimensional space of relevant CTQ responses that best separated yes/no respondents
to each ACE item. This effectively transformed the CTQ in a manner that differentially weighed
the contributions of various items; this may be important due to imperfect semantic mappings
between questionnaires. We implemented linear SVM (using v 6.0-84 in caret R). We selected
values of , a cost/penalty parameter, that returned the greatest accuracy in the discovery sampl C e
(out of .75, .9, 1, 1.1, and 1.25; emotional abuse=1.1, physical abuse=1.1, sexual abuse=.9,
emotional neglect=1.25, physical neglect=1). While larger values of increase accuracy, they C
may overfit the data; we therefore reassess correspondence in a separate validation sample.
Correspondence Metrics
For all approaches, we calculated metrics commonly used to assess the effectiveness of
medical diagnostic tests, including accuracy, sensitivity, and specificity. Sensitivity reflects the
true positive rate—i.e., the proportion of participants with correctly predicted ACE endorsements
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
out of all actual endorsements. Specificity reflects the true negative rate—i.e., the proportion of
participants with correctly predicted ACE non-endorsements out of the actual non-endorsements.
We plotted the true positive versus false positive rates for all possible subscale-based
thresholds and for each maltreatment type. From these ROC plots, we calculated the area under the curve (using v 2.2.1 in plotROC
R), which estimates the ability to detect concurrent ACE
endorsement from summed CTQ scores. See Supplementary Table 2 for the number of true/false
positives and negatives, as well as positive and negative predictive values. Results and Discussion
This brief methodological report aimed to evaluate the correspondence between the ACE
questionnaire and the CTQ. Across five types of maltreatment, we used diverse approaches to
transform continuous CTQ responses to binary predicted ACE endorsements. We then evaluated
the correspondence of these transformations to actual endorsements on the ACE questionnaire.
CTQ to ACE Questionnaire Correspondence
Across thresholding approaches, averaged accuracy ranged from 81.5-90.6%, averaged
sensitivity ranged from 52.3-86.3%, and averaged specificity ranged from 80.6-96.6% (discovery
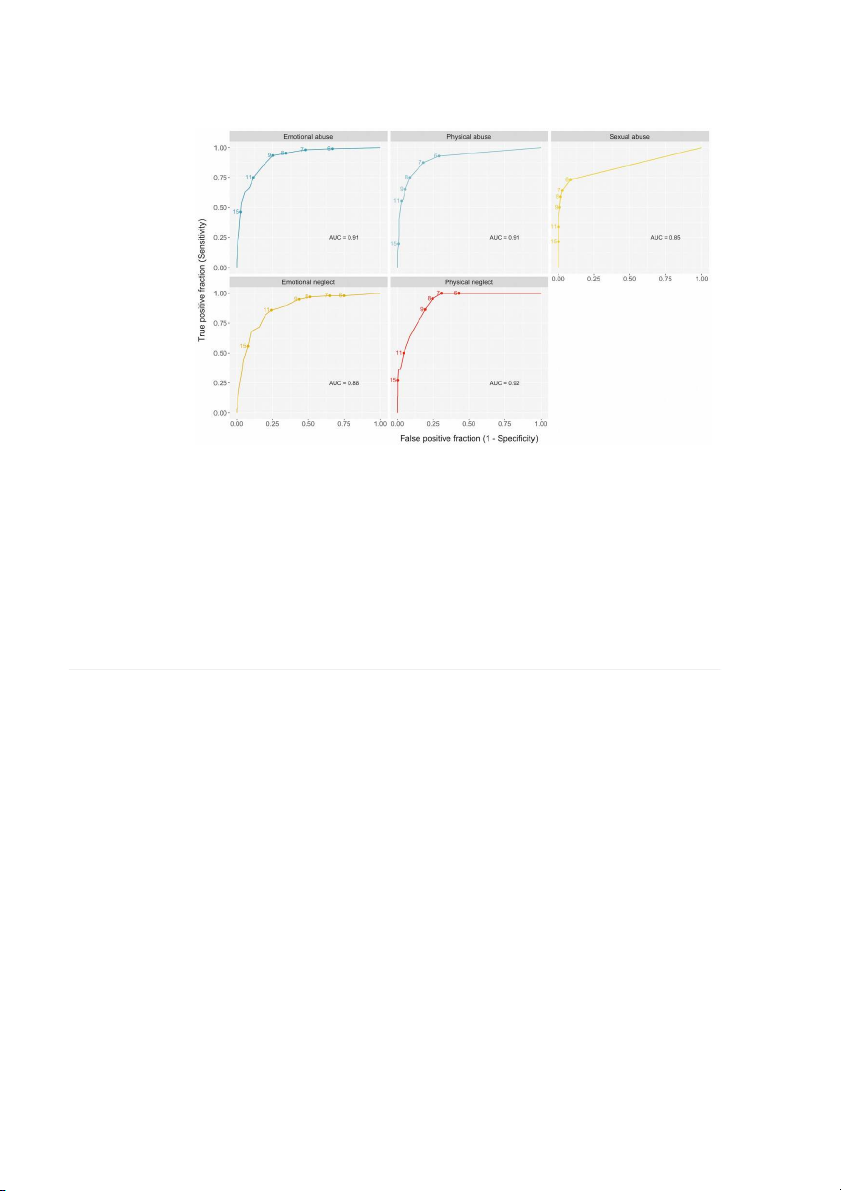
sample; Figure 1A; physical neglect was excluded as discussed below). In ROC plots, the area
under the curve ranged from 0.85-0.92 across maltreatment types (Figure 2). Physical neglect
exhibited some of the worst and most variable correspondence metrics (Figure 1B; discovery
sample accuracy=76.2-96.4%, sensitivity=31.8-95.5%, specificity=75.2-99.6%). This might be
partly explained by a unique feature of the physical neglect ACE item; for physical neglect only,
the list of experiences comprising the ACE item is joined by “and” instead of “or,” implying that
endorsement should only follow if all experiences occurred. Perhaps relatedly, only 22
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
participants endorsed this item. This may also reflect the moderately high socioeconomic status
of the sample (suggested by parental education; Table 1). Together, results suggest moderate to
strong correspondence across questionnaires for four of five maltreatment types in this sample.
Evaluating Thresholding Approaches
Item-based thresholding performed relatively poorly across correspondence metrics
(Figure 1A), which might be attributed to differences in the wording of the two questionnaires or
other measurement errors. The remaining thresholding approaches resulted in different
tendencies with respect to typical trade-offs between sensitivity and specificity (Figure 1).
Subscale-based thresholds determined by Youden’s Index generally had relatively higher
sensitivity and lower specificity but the lowest accuracies (due to lower base rates of adversity).
Support vector machine analyses generally resulted in the highest accuracy and specificity, but at
some cost to sensitivity. In comparison to this approach, subscale-based thresholds set by the
fixed cost-benefit ratio tended to have slightly decreased accuracy and specificity (<1% and
3.4% differences, respectively, across maltreatment types excluding physical neglect), but higher
sensitivity values (11.4% difference across maltreatment types excluding physical neglect) in the
discovery sample. Due to the greater difficulty of implementing machine learning, this subscale-
based approach might be most appropriate when seeking to reduce the number of
misclassifications while maintaining adequate sensitivity and specificity.
Due to space constraints, results for many thresholding approaches are not shown. We
created an interactive Shiny App for interested readers to explore results at multiple thresholds
(https://theresacheng.shinyapps.io/ctq_to_aces_shiny; see Supplementary Figure 1 for a preview
of the app; code available at https://github.com/theresacheng/ctq_to_aces_shiny).
Evaluating Generalization to a Validation Sample
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
All approaches except item-based thresholding involved threshold selection or parameter-
tuning using algorithms (conducted in the discovery sample only). Therefore, it was essential to
evaluate performance in a separate validation sample. Results suggest comparable accuracy
levels and a tendency to identify improved sensitivity and worse specificity in the validation
sample. Overall, no evidence suggests significant overfitting (Figure 1). Limitations
Our young adult samples over-represent White and middle-class participants (suggested
by high parental education levels; Table 1), limiting generalizability. Retrospective self-reports
of maltreatment were not corroborated (e.g., by therapist ratings), and analyses cannot speak to
associations with other measures of childhood adversity. Summary
This brief methodological report assists researchers in understanding the comparability of
maltreatment measures on two common childhood adversity self-report questionnaires. Overall,
we found somewhat good correspondence between the CTQ and ACE questionnaires for four of
five types of maltreatment. Correspondent metrics were worse overall for physical neglect and
highly variable across thresholding approaches. In considering the goals of (a) reducing the
overall number of misclassifications, (b) maintaining both sensitivity and specificity, and (c) ease
of use, results suggest that subscale-based thresholds selected via a fixed cost-benefit ratio may
be the most ideal, on balance. Results speak to the potential to pool participants for secondary
analyses; making full use of available data is of interest because it can be resource-intensive to
recruit high adversity samples and to manage legal and ethical responsibilities that arise when
asking adults or minors about significant past or ongoing adversities.
ADVERSITY QUESTIONNAIRE CORRESPONDENCE References
Bernstein, D. P., Ahluvalia, T., Pogge, D., & Handelsman, L. (1997). Validity of the Childhood
Trauma Questionnaire in an adolescent psychiatric population. Journal of the American
Academy of Child and Adolescent Psychiatry, 36(3), 340–348.
https://doi.org/10.1097/00004583-199703000-00012
Bernstein, David P, Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., Stokes,
J., Handelsman, L., Medrano, M., Desmond, D., & Zule, W. (2003). Development and
validation of a brief screening version of the Childhood Trauma Questionnaire. Child
Abuse & Neglect, 27(2), 169–190. https://doi.org/10.1016/S0145-2134(02)00541-0
Cortes, C., & Vapnik, V. (1995). Support-vector networks. Machine Learning, (3), 273–297. 20
https://doi.org/10.1007/BF00994018
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss,
M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction
to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. ,
American Journal of Preventive Medicine 14(4), 245–258.
Gilbert, L. K., Breiding, M. J., Merrick, M. T., Thompson, W. W., Ford, D. C., Dhingra, S. S., &
Parks, S. E. (2015). Childhood Adversity and Adult Chronic Disease. American Journal
of Preventive Medicine, 48(3), 345–349. https://doi.org/10.1016/j.amepre.2014.09.006
McNeil, B. J., Keller, E., & Adelstein, S. J. (1975). Primer on certain elements of medical decision making. ,
The New England Journal of Medicine (5), 211–215. 293
https://doi.org/10.1056/NEJM197507312930501
Smits, N. (2010). A note on Youden’s J and its cost ratio. BMC Medical Research Methodology,
10, 89. https://doi.org/10.1186/1471-2288-10-89
Teicher, M. H., & Parigger, A. (2015). The “Maltreatment and Abuse Chronology of Exposure”
(MACE) scale for the retrospective assessment of abuse and neglect during development.
PloS One, 10(2), e0117423. https://doi.org/10.1371/journal.pone.0117423
ADVERSITY QUESTIONNAIRE CORRESPONDENCE Table 1
Sociodemographic comparison of training and validation samples Measures Training sample Validation sample Gender 273 female; 198 male 43 female; 21 male Age (years ± SD) 22.8 ± 1.7 19.1 ± 0.5 Race American Indian 8 (1.7%) 0 (0%) Asian 65 (13.8%) 9 (14.1%) Black 43 (9.1%) 7 (10.9%) Other/Multiracial 27 (5.7%) 5 (7.8%) White 326 (69.2%) 43 (67.2%) Unknown 2 (0.4%) 0 (0%) Ethnicity Hispanic 49 (10.4%) 7 (10.8%) Not Hispanic 420 (89.2%) 58 (89.2%) Unknown 2 (0.4%) 0 (0%)
Parental education (years ± SD) 15.8 ± 3.1 15.3 ± 3.1
Endorsed maltreatment on the ACE questionnaire Emotional abuse 108 (22.9%) 31 (48.4%) Physical abuse 72 (15.3%) 19 (29.7%) Sexual abuse 56 (11.9%) 11 (17.2%) Emotional neglect 99 (21.0%) 24 (37.5%) Physical neglect 22 (4.7%) 11 (17.2%)
ADVERSITY QUESTIONNAIRE CORRESPONDENCE
Figure 1. Correspondence metrics by thresholding procedure for discovery and validation
samples. Panel (A) shows accuracy, sensitivity, specificity and specificity collapsed across
maltreatment types, while panel (B) separates out this information for each maltreatment type.
Figure 2. Receiver operating characteristic (ROC) plots for each maltreatment type in the discovery dataset. Examination of area
under the curve (AUC) estimates the ability to detect ACE endorsement from summed scores of relevant CTQ items. At the extremes,
a line at a 45-degree angle (AUC=0.5) indicates that signal cannot be distinguished from noise (no correspondence), while a curve that
hugs the upper left-hand corner of the plot (AUC = 1) indicates perfect correspondence. Supplementary Materials Supplementary Table 1
Language discrepancies between the ACE questionnaire and CTQ Adversity ACE questionnaire item CTQ item themesa Discrepanciesb Emotional
“Did a parent or other adult in the household
Being called names, insulted, or
- The CTQ items do not address the Abuse
often…Swear at you, insult you, put you
feeling hated or unwanted by family
second clause of the ACE question
down, or humiliate you? -or- Act in a way that
members; self-identification as a
indicating fear of physical harm.
made you afraid that you might be physically victim of emotional abuse hurt?" Physical
“Did a parent or other adult in the household
Being physically hit or punished to a
- The CTQ specifies that physical harm Abuse
often…Push, grab, slap, or throw something at
noticeable degree, with certain
includes the use of marks or hard objects,
you? -or- Ever hit you so hard that you had objects, or requiring medical
suggesting a somewhat higher level of marks or were injured?”
attention; self-identification as a physical intensity. victim of physical abuse Sexual
“Did an adult or person at least 5 years older
Having had someone else try to
- The ACE item specifies that the person Abuse
than you ever…Touch or fondle you or have
engage in sexual activities with them; is an adult or 5+ years older
you touch their body in a sexual way? -or- Try
experiencing physical or emotional
- The CTQ includes sexual coercion and
to or actually have oral, anal, or vaginal sex
threats as a means of sexual coercion;
sexual acts that occur without physical with you?”
self-identification as a victim of contact. molestation and sexual abuse. Emotional
“Did you often feel that… No one in your
Not feeling important, special, loved,
- Each item of the CTQ phrased similarly, Neglect
family loved you or thought you were
cared for, supported, and lacking but is reverse scored.
important or special? -or- Your family didn’t
high-quality relationships with family
look out for each other, feel close to each members.
other, or support each other?” Physical
“Did you often feel that… You didn’t have
Lacking in basic necessities (e.g.,
- Two CTQ items are reverse scored. Neglect
enough to eat, had to wear dirty clothes, and
food, clothing, access to medical
- The ACE items are joined by “and”;
had no one to protect you? -or- Your parents
care); not having an available
participants might only endorse if all
were too drunk or high to take care of you or
caretaker; parental substance abuse three are true.
take you to the doctor if you needed it?”
issues that interfere with child care
a wording of CTQ items is not printed due to copyright issues b CTQ also directly addresses belief about the occurrence of each type of abuse. Supplementary Table 2
Comparison of thresholding methods in the discovery sample Number of subjects Metrics (in %) Thresholds True + True - False + False - Sensitivity Specificity + Predictive - Predictive Value Value Item-based EA 4 (Often True) 74 324 37 34 68.5 89.8 66.7 90.5 PA 4 (Often True) 35 366 26 37 48.6 93.4 57.4 90.8 SA 2 (Rarely True) 41 378 35 15 73.2 91.5 54.0 96.2 EN 4 (Often True) 68 292 79 31 68.7 78.7 46.3 90.4 PN 4 (Often True) 13 384 64 9 59.1 85.7 16.9 97.7 Subscale-based: Youden Index EA 9 (Low/Mod) 100 264 89 7 93.5 74.8 52.9 97.4 PA 7 (None/Min) 63 313 70 9 87.5 81.7 47.4 97.2 SA 6 (Low/Mod) 41 369 35 15 73.2 91.3 53.9 96.1 EN 12 (Low/Mod) 81 291 72 17 82.7 80.2 52.9 94.5 PN 8 (Low/Mod) 21 333 106 1 95.5 75.9 16.5 99.7 Subscale-based: Cost-Benefit EA 11 (Low/Mod) 81 319 42 27 75.0 88.4 65.9 92.2 PA 8 (Low/Mod) 54 358 34 18 75.0 91.3 61.4 95.2 SA 7 (Low/Mod) 36 401 12 20 64.3 97.1 75.0 95.3 EN 14 (Low/Mod) 67 334 37 32 67.7 90.0 64.4 91.3 PN 14 (Sev/Ext) 8 445 3 14 36.4 99.3 72.7 97.0
Subscale-based: CTQ Low to Moderate Severity Cutoff EA 9 (Low/Mod) 101 270 91 7 93.5 74.8 52.6 97.5 PA 8 (Low/Mod) 54 358 34 18 75.0 91.3 61.4 95.2 SA 6 (Low/Mod) 41 378 35 15 73.2 91.5 54.0 96.2 EN 10 (Low/Mod) 88 249 122 11 82.7 80.2 52.9 94.5 PN 8 (Low/Mod) 21 338 110 1 95.5 75.5 16.0 99.7
Support Vector Machine Learning EA C = 1.1 69 338 23 39 63.9 93.6 75 89.7 PA = 1.1 C 39 382 10 33 54.2 97.4 79.6 92 SA = .9 C 33 406 7 23 58.9 98.3 82.5 94.6 EN C = 1.25 52 349 22 47 52.5 94.1 70.3 88.1 PN = 1 C 7 446 2 15 31.8 99.6 77.8 96.7
Note: Maltreatment type abbreviations are emotional abuse (EA), physical abuse (PA), sexual abuse (SA), emotional neglect (EN),
and physical neglect (PN). Item-based thresholds are described in terms of frequency, while all other thresholds are contextualized by
severity categories as described in the manual for the Childhood Trauma Questionnaire (Bernstein & Fink, 1997), as follows: none or
minimal (None/Min), low to moderate (Low/Mod), moderate to severe (Mod/Sev), and severe to extreme (Sev/Ext). Positive is
abbreviated as (+) and negative is abbreviated as (-) for both true/false positives and negatives, as well as positive and negative
predictive values. We caution against interpreting positive and negative predictive values, as they would be strongly contingent on
prevalence and rates of adversity were intentionally sampled in both the discovery and validation samples. For the support vector
machine learning approach, the cost/penalty parameter is abbreviated
In addition to the thresholding approaches described in the C.
manuscript, we additionally examined the threshold between none or minimal and low to moderate exposure as defined by Bernstein
and Fink (1997), as this theoretically demarcates participants who have/have not experienced childhood maltreatment.
Tài liệu liên quan:
-

Development and validation of a brief sc - Tài liệu tham khảo | Đại học Hoa Sen
282 141 -

Adverse Childhood Experiences (ACE) Study - Tài liệu tham khảo | Đại học Hoa Sen
359 180 -

Relationship Between Emotional Neglect of Parents and Children’s Internalizing, Externalizing Behavior Problems and Academic Achievement
74 37 -

Adverse ChildhoodExperiences (ACEs) - Tài liệu tham khảo | Đại học Hoa Sen
345 173