Tài liêu ôn tập. Chương 7. Xử lí tổn thương bankart xương
Tài liêu ôn tập. Chương 7. Xử lí tổn thương bankart xương. Tài liệu được tổng hợp và sưu tầm gồm 9 trang. Mời các bạn tham khảo
Môn: Tài liệu Tổng hợp 3.6 K tài liệu
Trường: Tài liệu khác 3.9 K tài liệu
Tác giả:
Preview text:
Chương 7: “Xử trí tổn thương Bankart xương/Mất xương ổ chảo: Kỹ thuật Latarjet nội soi”
Abstract Latarjet procedure, no matter open or arthroscopic, is an excellent and reliable technique in restoring anterior shoulder stability. Compared with open technique, arthroscopic Latarjet procedure has several advantages including more accurate graft placement, simultaneous management of associated shoulder pathologies, less risk of postoperative shoulder stiffness, faster rehabilitation, and cosmetic benefits. The extent of glenoid bone loss is the major factor when considering whether to perform a Latarjet procedure. Meanwhile, patient’s age, the presence of humeral bone loss, history of failed arthroscopic Bankart repair, and patient’s lifestyle should also be taken into consideration when making surgical plan. Common operative complications of Latarjet procedure are graft bone resorption/osteolysis, bone block non union, graft fracture, neurovascular injury, and osteoarthritis. Given the steep learning curve with arthroscopic Latarjet procedure, it should be performed by experienced arthroscopy surgeons. Keywords Arthroscopic · Latarjet · Bristow · Coracoid transfer. Glenoid bone loss · Bony Bankart · Anterior shoulder instability · Outcomes · Complications | Tóm tắtKỹ thuật Latarjet, dù thực hiện bằng mổ mở hay nội soi, đều là một phương pháp tuyệt vời và đáng tin cậy trong việc phục hồi sự vững khớp vai trước. So với kỹ thuật mổ mở, phương pháp Latarjet nội soi có nhiều ưu điểm, bao gồm đặt mảnh ghép chính xác hơn, xử trí đồng thời các bệnh lý đi kèm của khớp vai, giảm nguy cơ cứng khớp vai sau mổ, phục hồi nhanh hơn và mang lại lợi ích thẩm mỹ. Mức độ mất xương ổ chảo là yếu tố quan trọng nhất khi cân nhắc có nên thực hiện kỹ thuật Latarjet hay không. Bên cạnh đó, tuổi bệnh nhân, sự hiện diện của mất xương chỏm cánh tay, tiền sử thất bại của phẫu thuật Bankart nội soi trước đó và lối sống của bệnh nhân cũng cần được xem xét khi lập kế hoạch phẫu thuật. Các biến chứng thường gặp của phẫu thuật Latarjet bao gồm tiêu xương/ly giải mảnh ghép, không liền khối xương ghép, gãy mảnh ghép, tổn thương thần kinh–mạch máu và thoái hóa khớp. Do đường cong học kỹ thuật của phương pháp Latarjet nội soi khá dốc, thủ thuật này nên được thực hiện bởi các phẫu thuật viên nội soi có kinh nghiệm. Từ khóaNội soi · Latarjet · Bristow · Chuyển mỏm quạ · Mất xương ổ chảo · Tổn thương Bankart xương · Mất vững khớp vai trước · Kết quả · Biến chứng |
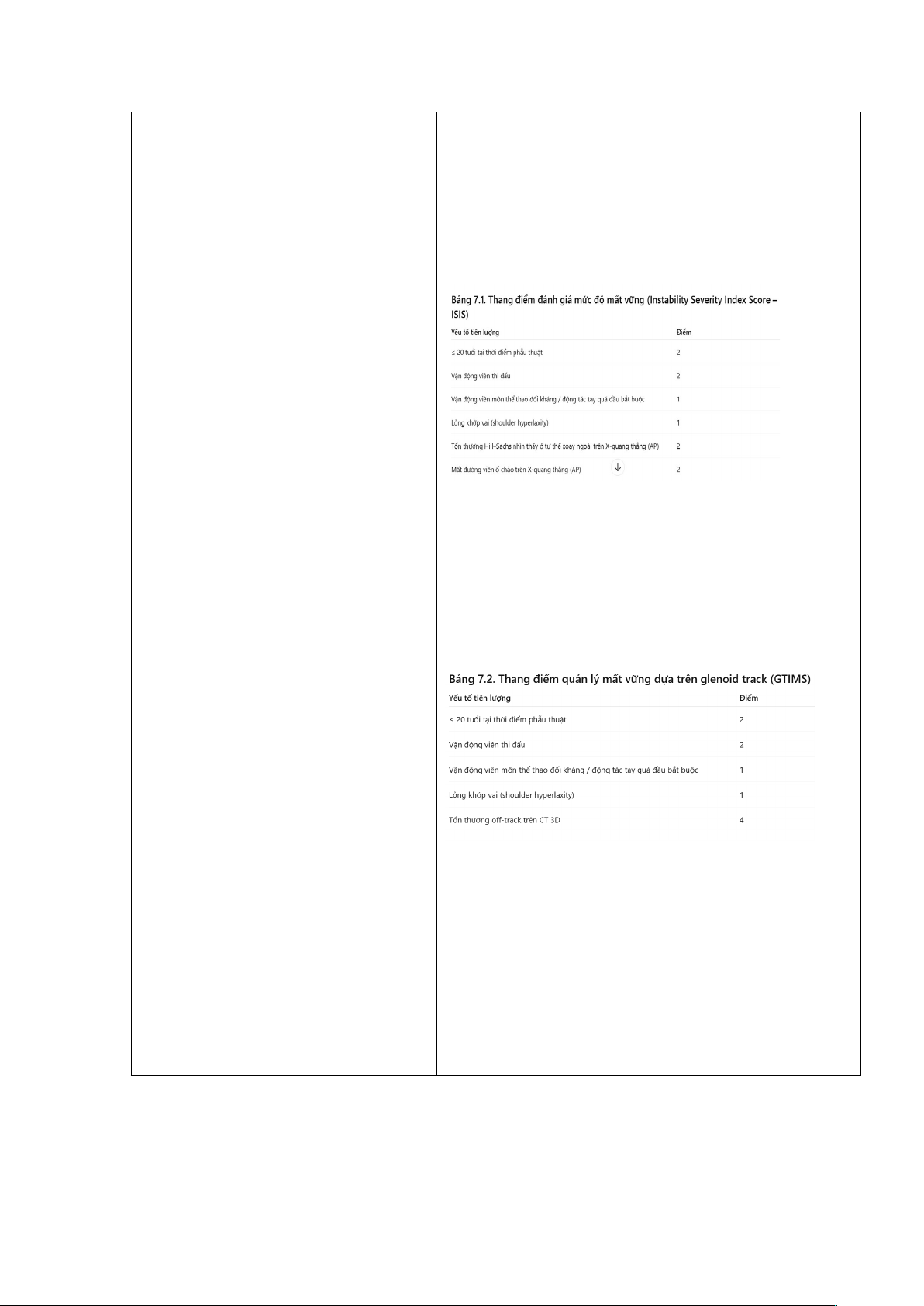
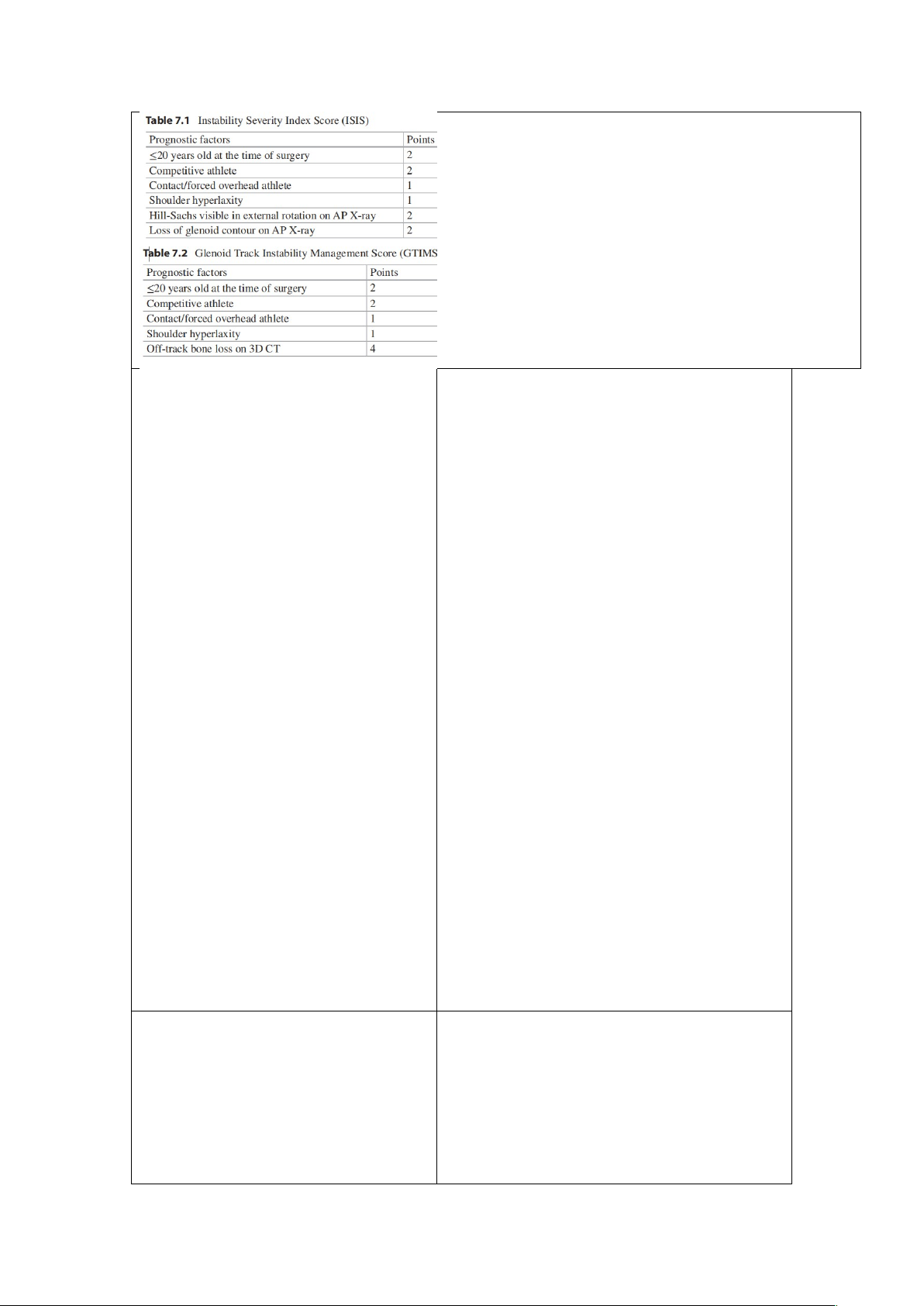
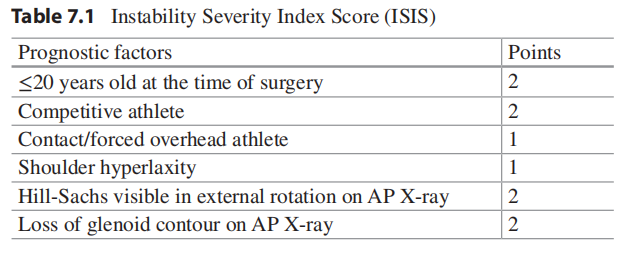
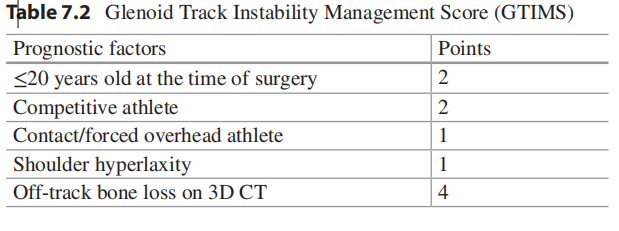
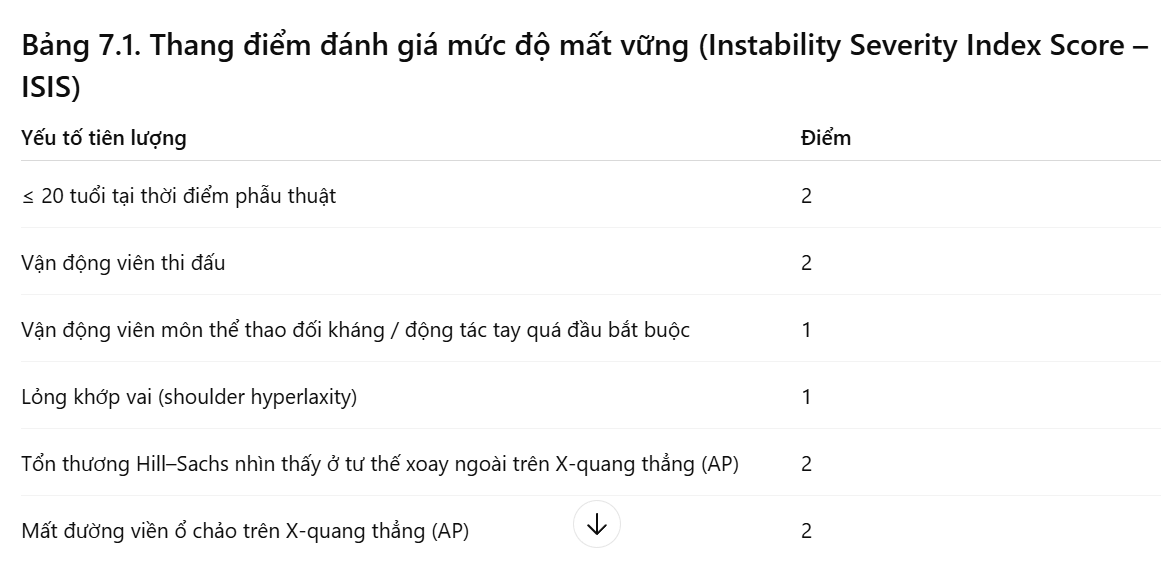
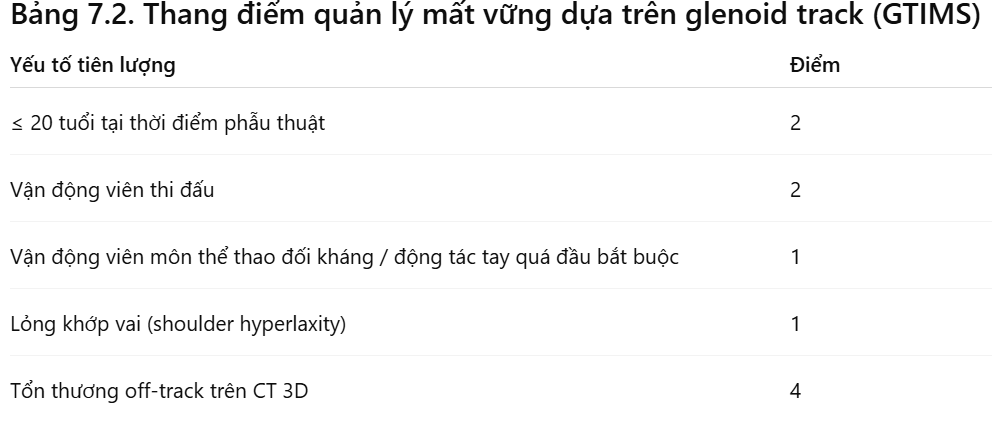
7.1 Introduction Arthroscopic Bankart repair is the most used surgical technique for the treatment of anterior shoulder instability. For patients without significant glenoid bone defects, the success rate of arthroscopic Bankart repair is 96% [1]. However, it has been reported that 22% of first-time anterior shoulder dislocation patients possess some degree of glenoid bone loss [2], and this proportion increases to 76% in recurrent cases [3–5]. For this group of patients, the failure rate of Bankart repair reaches to as high as 67–89% [1], indicating that an alternative surgical procedure is necessary for these cases. Coracoid transfer (Latarjet/Bristow procedure) was first introduced by Latarjet in 1954 to treat patients with significant glenoid bone deficiency. In this procedure, the coracoid bone block, along with the conjoint tendon, is brought into the joint through a subscapularis split and fixed to the glenoid neck. The major differences between Latarjet and Bristow procedure are the length and position of the osteomized coracoid. While Bristow procedure uses a shorter coracoid and fixes it perpendicular to the glenoid with only one screw, Latarjet procedure uses a longer bone segment and fixes it parallel to the glenoid with two screws. In spite of these discrepancies, the stabilizing mechanisms of these two procedures are almost the same: (1) the transferred coracoid acts to increase the anterior diameter of the glenoid, (2) the transferred conjoint tendon adds tension to the inferior portion of the subscapularis when the arm is abducted and externally rotated, thus creating a dynamic sling to reinforce the anteroinferior capsule, (3) repair of the capsuloligamentous complex to the glenoid re-tensions the anteroinferior capsule [6]. The open Latarjet procedure has been proved to be an excellent and reliable technique in restoring shoulder stability [7–10]. In 2003, Lafosse began to perform it under arthroscopy and published the first technical report of arthroscopic Latarjet procedure in 2007 [11]. Compared with open procedure, the arthroscopic Latarjet/Bristow offers many advantages including more accurate graft placement, simultaneous management of associated shoulder pathologies, less risk of postoperative shoulder stiffness, faster rehabilitation, and cosmetic benefits [12]. Since then, increasing shoulder surgeons changed from an open to an arthroscopic procedure, and comparable clinical outcomes and complication rates have been reported between open and arthroscopic Latarjet techniques [13–15]. 7.2 Indications The extent of glenoid bone loss is the major factor when considering whether to perform an arthroscopic Latarjet procedure. Meanwhile, patient’s age, the presence of humeral bone loss, history of failed arthroscopic Bankart repair, and patient’s lifestyle should also be taken into consideration when making surgical plan. As stated previously, severe glenoid bone loss is the biggest risk factor for recurrence following arthroscopic Bankart repair, with failure rate of up to 67–89% [1]. Nevertheless, the threshold of critical glenoid bone loss has always been a topic of controversy. Di Giacomo et al. initially suggested that patients with more than 25% of glenoid bone loss are appropriate candidates for osseous reconstruction surgery [16]. Lower thresholds as 13.5–15% have been recom mended by more recent publications [17–19]. The glenoid track concept, by taking both humeral and glenoid bone loss into consideration, provides useful guide regarding whether an additional remplissage or osseous block procedure is necessary [16]. For patients with critical glenoid bone loss and an off-track Hill-Sachs lesion, a Latarjet with or without remplissage procedure is indicated. And for patients with subcritical glenoid bone loss and concomitant off-track Hill-Sachs lesion, the Latarjet procedure may provide improved stability than Bankart repair plus remplissage [20]. The Instability Severity Index Score (ISIS) was developed by Pascal Boileau to screen for patients appropriate for Latarjet procedure (Table 7.1). In this 10-point scoring system, patients with a score over 6 points had an unacceptable recurrence risk of 70% after arthroscopic Bankart repair and were believed good candidates of osseous reconstruction procedure [21]. Quite recently, the Glenoid Track Instability Management Score (GTIMS) was introduced [22]. Compared with ISIS, GTIMS relies on three-dimensional computed tomography (CT) scan, rather than plain radiographs, to evaluate glenoid and humeral bone deficiency (Table 7.2). For both scoring systems, a score of >4 points suggests the necessity of an osseous reconstruction [22, 23].
| 7.1 Giới thiệuKhâu Bankart nội soi là kỹ thuật phẫu thuật được sử dụng nhiều nhất trong điều trị mất vững khớp vai trước. Đối với bệnh nhân không có thiếu hụt đáng kể xương ổ chảo, tỷ lệ thành công của khâu Bankart nội soi lên đến 96% [1]. Tuy nhiên, đã có báo cáo rằng 22% bệnh nhân trật khớp vai trước lần đầu có một mức độ nào đó mất xương ổ chảo [2], và tỷ lệ này tăng lên đến 76% ở những trường hợp tái hồi [3–5]. Với nhóm bệnh nhân này, tỷ lệ thất bại của phẫu thuật Bankart có thể cao đến 67–89% [1], cho thấy cần có một phương pháp phẫu thuật thay thế. Kỹ thuật chuyển mỏm quạ (Latarjet/Bristow) được Latarjet giới thiệu lần đầu vào năm 1954 nhằm điều trị các bệnh nhân có thiếu hụt đáng kể xương ổ chảo. Trong kỹ thuật này, mảnh xương mỏm quạ cùng với gân chung được đưa vào khớp thông qua một đường tách cơ dưới vai và được cố định vào cổ ổ chảo. Sự khác biệt chính giữa kỹ thuật Latarjet và Bristow nằm ở chiều dài và vị trí của đoạn xương được cắt. Kỹ thuật Bristow sử dụng một đoạn mỏm quạ ngắn hơn và cố định vuông góc với ổ chảo bằng một vít, trong khi kỹ thuật Latarjet sử dụng một đoạn xương dài hơn và cố định song song với ổ chảo bằng hai vít. Mặc dù có những khác biệt này, cơ chế tạo vững của cả hai kỹ thuật gần như giống nhau:
7.2 Chỉ địnhMức độ mất xương ổ chảo là yếu tố quan trọng nhất khi cân nhắc có nên thực hiện phẫu thuật Latarjet nội soi hay không. Bên cạnh đó, tuổi bệnh nhân, sự hiện diện của mất xương chỏm cánh tay, tiền sử thất bại của phẫu thuật Bankart nội soi trước đó và lối sống của bệnh nhân cũng cần được xem xét khi lập kế hoạch phẫu thuật. Như đã nêu trước đây, mất xương ổ chảo nặng là yếu tố nguy cơ lớn nhất gây tái phát sau phẫu thuật Bankart nội soi, với tỷ lệ thất bại lên đến 67–89% [1]. Tuy nhiên, ngưỡng “mất xương ổ chảo tới hạn” luôn là chủ đề gây tranh cãi. Di Giacomo và cộng sự ban đầu đề xuất rằng bệnh nhân có mất hơn 25% xương ổ chảo là đối tượng phù hợp để thực hiện phẫu thuật tái tạo xương [16]. Những nghiên cứu gần đây hơn đã đề xuất ngưỡng thấp hơn, khoảng 13.5–15% [17–19]. Khái niệm glenoid track, bằng cách tính đến cả mất xương chỏm cánh tay và ổ chảo, cung cấp hướng dẫn hữu ích về việc có cần thực hiện thêm thủ thuật remplissage hoặc phẫu thuật ghép xương hay không [16]. Ở những bệnh nhân có mất xương ổ chảo tới hạn kèm tổn thương Hill-Sachs off-track, chỉ định thực hiện Latarjet có hoặc không kèm remplissage. Ở bệnh nhân có mất xương ổ chảo dưới ngưỡng tới hạn nhưng có Hill-Sachs off-track, phẫu thuật Latarjet có thể đem lại độ vững tốt hơn so với Bankart + remplissage [20]. Thang điểm Instability Severity Index Score (ISIS) do Pascal Boileau phát triển nhằm sàng lọc bệnh nhân phù hợp cho phẫu thuật Latarjet (Bảng 7.1). Trong hệ thống 10 điểm này, bệnh nhân có trên 6 điểm sẽ có nguy cơ tái phát 70% sau Bankart nội soi và được xem là ứng viên phù hợp cho phẫu thuật tái tạo xương [21].
Gần đây hơn, thang điểm Glenoid Track Instability Management Score (GTIMS) đã được giới thiệu [22]. So với ISIS, GTIMS dựa vào CT scan 3D, thay vì X-quang thường, để đánh giá mức độ mất xương ổ chảo và chỏm cánh tay (Bảng 7.2).
| |
7.3 Contraindications Patients with uncontrolled epilepsy are absolutely contraindicated for the Latarjet procedure because any recurrence of seizures can lead to coracoid graft fracture. Complete neurological stability is mandatory before treating recurrent shoulder dislocation in epileptic patients [24]. Voluntary dislocators are also absolute contraindications to the Latarjet procedure because surgery is not able to correct soft tissue laxity. The surgical outcomes for this group of patients are extremely poor and conservative therapy should be the first choice of treatment. Chronic locked anterior dislocation should not be treated with Latarjet procedure because of the risk of redislocation. Conservative treatment or reverse shoulder arthroplasty is advised for this kind of patients. | 7.3 Chống chỉ địnhBệnh nhân động kinh không được kiểm soát là chống chỉ định tuyệt đối của phẫu thuật Latarjet vì bất kỳ cơn co giật tái phát nào cũng có thể dẫn đến gãy mảnh ghép mỏm quạ. Do đó, ổn định thần kinh hoàn toàn là điều bắt buộc trước khi điều trị tình trạng trật khớp vai tái diễn ở bệnh nhân động kinh [24]. Những bệnh nhân tự chủ động trật khớp vai (voluntary dislocators) cũng là chống chỉ định tuyệt đối đối với phẫu thuật Latarjet, vì phẫu thuật không thể điều chỉnh tình trạng lỏng lẻo mô mềm. Kết quả phẫu thuật ở nhóm này rất kém và điều trị bảo tồn phải là lựa chọn ưu tiên. Tình trạng trật khớp vai trước mạn tính cố định (chronic locked anterior dislocation) không nên điều trị bằng kỹ thuật Latarjet vì nguy cơ tái trật cao. Điều trị bảo tồn hoặc thay khớp vai ngược (reverse shoulder arthroplasty) được khuyến cáo cho nhóm bệnh nhân này. | |
7.4 Related Anatomy The risk of neurovascular injury during arthroscopic Latarjet procedure is being reported to be 1.6% [25]. The nerves primarily at risk are the axillary nerve, the musculocutaneous nerve, and the suprascapular nerve. Thus, it is crucial to remember in heart the detailed anatomy of neurovascular bundles in this region. The musculocutaneous nerve is at the highest risk. It is the terminal branch of the lateral cord of the brachial plexus and enters the coracobrachialis muscle after passing the inferior border of pectoralis minor muscle. Injury to this nerve can occur during coracoid preparation and passage of the coracoid through the subscapularis split. Careful blunt dissection and exposure are important to prevent injury to this nerve. The axillary nerve originates as a terminal branch of the posterior cord of the brachial plexus. It descends posterior to the axillary artery and anterior to the subscapularis. It is at risk especially during subscapularis split and the passage of the coracoid graft. In a cadaveric study, Hawi et al. found that in 50% of shoulders studied, the axillary nerve is just located within the subscapularis split and prone to injury [26]. Reinares et al. have demonstrated that externally rotating the scapula could increase the distance between the axillary nerve and coracoid fixation screw, thus decreasing the risk of injury [27]. The suprascapular nerve travels around the base of the scapular spine from anterior to posterior, then courses medially and downwardly into the infraspinatus muscle. It is at risk for injury during screw fixation of the coracoid to the glenoid [28]. To avoid its injury, the fixation screw should aim as lateral as possible, no more than 2.1 cm medial to the posterior glenoid articular surface [28]. | 7.4 Giải phẫu liên quanNguy cơ tổn thương thần kinh–mạch máu trong quá trình thực hiện phẫu thuật Latarjet nội soi được báo cáo khoảng 1.6% [25]. Các dây thần kinh có nguy cơ cao nhất bao gồm dây thần kinh nách (axillary nerve), dây cơ bì (musculocutaneous nerve) và dây trên vai (suprascapular nerve). Vì vậy, việc nắm vững chi tiết giải phẫu của các bó mạch–thần kinh trong vùng này là hết sức quan trọng. Dây cơ bì (musculocutaneous nerve)Đây là dây thần kinh có nguy cơ cao nhất bị tổn thương. Nó là nhánh tận của bó ngoài đám rối cánh tay và đi vào cơ quạ–cánh tay (coracobrachialis) sau khi đi qua bờ dưới cơ ngực bé (pectoralis minor). Dây thần kinh nách (axillary nerve)Dây thần kinh nách là nhánh tận của bó sau đám rối cánh tay. Nó đi xuống phía sau động mạch nách và phía trước cơ dưới vai. Trong một nghiên cứu trên xác, Hawi và cộng sự phát hiện rằng ở 50% mẫu, dây thần kinh nách nằm ngay trong đường tách cơ dưới vai, làm tăng nguy cơ tổn thương [26]. Reinares và cộng sự cho thấy rằng xoay ngoài xương bả vai có thể tăng khoảng cách giữa dây thần kinh nách và vít cố định mỏm quạ, từ đó giảm nguy cơ tổn thương [27]. Dây thần kinh trên vai (suprascapular nerve)Dây thần kinh này đi quanh nền gai xương bả vai từ trước ra sau, sau đó đi vào cơ dưới gai theo hướng vào trong và xuống dưới. Dây thần kinh trên vai có nguy cơ bị tổn thương trong quá trình bắt vít cố định mảnh mỏm quạ vào ổ chảo [28]. | |
7.5 Surgical Technique 7.5.1 Patient Positioning The patient is placed in the beach chair position with the trunk elevated 45°. 7.5.2 Portals Five portals are used for the arthroscopic Latarjet procedure (Fig. 7.1). The A portal is the standard posterior portal and is used for initial visualization. The D portal is the anterolateral portal positioned 1 cm lateral to the anterolateral corner of the acromion. The H portal is superior to the coracoid and is used for coracoid osteotomy. The I portal is in line with the conjoint tendon, just in midway between the coracoid and axillary fossa. The M portal is at the level of the axillary fold, about four fingers width medial to the axillary fossa. This portal is safe as long as the surgeon remains anterior to the pectoralis minor muscle. It is used to introduce the doublebarrel cannula for coracoid transfer and fixation. 7.5.3 Procedures The surgical procedures for the arthroscopic Latarjet were first described by Lafosse et al. in 2007 [11]. In general, it can be divided into five sequential steps: exposure, coracoid preparation, coracoid osteotomy, subscapularis split, and graft transfer and fixation. 7.5.3.1 Step One: Joint Evaluation and Exposure The intra-articular evaluation is started through the standard “soft-spot” A portal. Using outside-in technique, the anterolateral D portal is established, and a probe is introduced through the rotator interval. Intra-articular structures including the anteroinferior capsular laxity, glenoid bone loss, and humeral head defect are carefully inspected (Fig. 7.2a). Subsequently, the rotator interval is opened by a shaver or radiofrequency device. Anterior glenoid bone bed is exposed from 2 to 6 o’clock position by releasing anteroinferior capsulolabral tissue from the glenoid neck. To be able to repair the capsule at the end of surgery, the capsulolabral tissue should be thoroughly released from both the glenoid neck and the deep surface of subscapularis muscle belly. Then, a burr is used to abrade the glenoid neck to make a fresh bone surface for graft healing. The intended screw insertion sites (normally 4 and 5 o’clock) are marked with radiofrequency device (Fig. 7.2b). 7.5.3.2 Step Two: Coracoid Preparation The coracoacromial ligament is detached from the coracoid, and the lateral side of the conjoint tendon is released from the deltopectoral fascia. Advancing the arthroscope over the lateral edge of the conjoint tendon, the I and M portals could be established using outside-in technique with the aid of a spinal needle. It is crucial to stay anterior to the pectoralis minor muscle when localizing and creating the M portal. The space superficial to the conjoint tendon is created by a shaver. Switching the arthroscope to the I portal, the medial aspect of the coracoid can be accessed with instrumentation through the M portal. Detach the pectoralis minor from the medial side of the coracoid with a radiofrequency device. The musculocutaneous nerve lies close to the inferomedial aspect of the conjoint tendon. To avoid injury, blunt dissection, rather than radiofrequency or shaver, should be used when clearing the medial side soft tissue of the conjoint tendon. After all soft tissues are cleared from the superior and inferior aspects of the coracoid, the H portal is created with a spinal needle. 7.5.3.3 Step Three: Coracoid Drilling and Osteotomy Carefully identify the tip of the coracoid. Put the double coracoid drill guide through the H portal. Two 1.5 mm K wires are inserted parallelly in the drill guide; note that the distal wire should be no less than 5 mm proximal to the coracoid tip. To avoid lateral screw placement, the insertion site of the two wires should be between the middle and medial third of the width of the coracoid (2/3 lateral and 1/3 medial). After removing the drill guide, the holes are enlarged, tapped, and inserted with a “Top Hat” washer, using the previously placed K wire as a guide (Fig. 7.3). Before coracoid osteotomy, a stress riser is created using a burr at the base of the coracoid. The burr, delivered through the M and D portal respectively, could reach all sides of the coracoid base. Be careful that the burr site should be at least 5 mm away from the proximal coracoid washer to prevent inadvertent coracoid fracture. After completion of the circumferential stress riser, the osteotomy is performed from the H portal using a curved osteotome. Then, the plastic double-barrel cannula is introduced via the M portal and connected with the coracoid graft by two long holding screws. Once the coracoid graft is attached to the cannula, it can be moved freely, and its inferior aspect is ready to be decorticated with a burr from the D portal. | 7.5 Kỹ thuật phẫu thuật7.5.1 Đặt tư thế bệnh nhânBệnh nhân được đặt ở tư thế ghế bãi biển (beach-chair) với thân mình nâng lên 45 7.5.2 Các đường vào (Portals)Có 5 đường vào được sử dụng trong phẫu thuật Latarjet nội soi (Hình 7.1): Cổng A: cổng sau tiêu chuẩn, dùng để quan sát ban đầu. Cổng D: cổng trước–bên, đặt cách 1 cm bên ngoài góc trước–bên của mỏm cùng vai. Cổng H: nằm phía trên mỏm quạ, dùng cho thao tác cắt mỏm quạ. Cổng I: nằm trên đường thẳng với gân chung (conjoint tendon), ở giữa mỏm quạ và hõm nách. Cổng M: ở mức nếp nách, khoảng 4 ngón tay vào trong so với hõm nách. Cổng này an toàn miễn là phẫu thuật viên luôn làm việc phía trước cơ ngực bé. 7.5.3 Các bước phẫu thuậtKỹ thuật Latarjet nội soi được Lafosse mô tả đầu tiên năm 2007 [11]. 7.5.3.1 Bước 1: Đánh giá khớp và bộc lộQuan sát trong khớp bắt đầu qua cổng A (soft spot). Tiến hành đánh giá các cấu trúc trong khớp: Độ lỏng bao trước–dưới Mất xương ổ chảo Khuyết xương chỏm (Hill-Sachs) Mở rotator interval bằng shaver hoặc dao đốt RF. Để có thể khâu lại bao sau khi hoàn tất, cần giải phóng mô bao – sụn viền: khỏi cổ ổ chảo và khỏi mặt sâu cơ dưới vai. Tiếp theo, dùng burr làm mới cổ ổ chảo chuẩn bị cho ghép xương. 7.5.3.2 Bước 2: Chuẩn bị mỏm quạ Cắt dây chằng quạ–cùng vai (coracoacromial ligament).Giải phóng mặt bên của gân chung khỏi cân delta–ngực (deltopectoral fascia). Đưa nội soi dọc bờ ngoài gân chung, sau đó tạo cổng I và M bằng kỹ thuật outside-in. Quan trọng: luôn tạo cổng M phía trước cơ ngực bé để đảm bảo an toàn. Dùng shaver tạo khoang trên mặt nông của gân chung. Chuyển nội soi qua cổng I: Bộc lộ mặt trong mỏm quạ qua cổng M. Dùng dao đốt RF tách cơ ngực bé khỏi mặt trong mỏm quạ Dây thần kinh cơ bì nằm sát mặt dưới–trong của gân chung. 7.5.3.3 Bước 3: Khoan và cắt mỏm quạXác định chính xác chóp mỏm quạ. Đưa dẫn hướng khoan đôi (double coracoid drill guide) qua cổng H. Khoan hai kim K 1.5 mm song song. Lưu ý:Kim dưới phải nằm cách chóp mỏm quạ ≥ 5 mm.Vị trí khoan phải ở 1/3 trong – 2/3 ngoài chiều rộng mỏm quạ, để tránh đặt vít quá ngoài.Sau khi tháo dẫn hướng, mở rộng lỗ và đặt vòng “Top Hat” theo kim K dẫn đường (Hình 7.3). Tạo vùng yếu (stress riser) để chuẩn bị cắt:Dùng burr tạo rãnh mỏng quanh gốc mỏm quạ từ cổng M và D. Khoảng này phải cách vòng Top Hat ≥ 5 mm để tránh gãy mỏm quạ. Sau khi hoàn tất rãnh vòng quanh, thực hiện cắt mỏm quạ bằng dao cắt cong từ cổng H. Tiếp theo: Đưa ống đôi (double-barrel cannula) qua cổng M. Nối với mảnh mỏm quạ bằng hai vít giữ dài. Khi mỏm quạ được gắn vào cannula, có thể di chuyển tự do và mặt dưới sẽ được làm mới bằng burr từ cổng D. |
Tài liệu liên quan:
-
Ung dung game hoa trong cac chien dich MKT
31 16 -
Bao cao Chi so TMDT Viet Nam 2025
34 17 -
Thông tư quy định về việc phân quyền, phân cấp và phân định thẩm quyền quản lý nhà nước về giáo dục cho chính quyền địa phương
37 19 -

Nghị quyết về phát huy các giá trị di sản văn hóa gắn với phát triên du lịch bền vững tỉnh Khánh Hòa đến năm 2025, định hướng đến năm 2030
36 18 -

Quyết định phê duyệt Chiến lược phát triển du lịch Việt Nam đến năm 2030
24 12