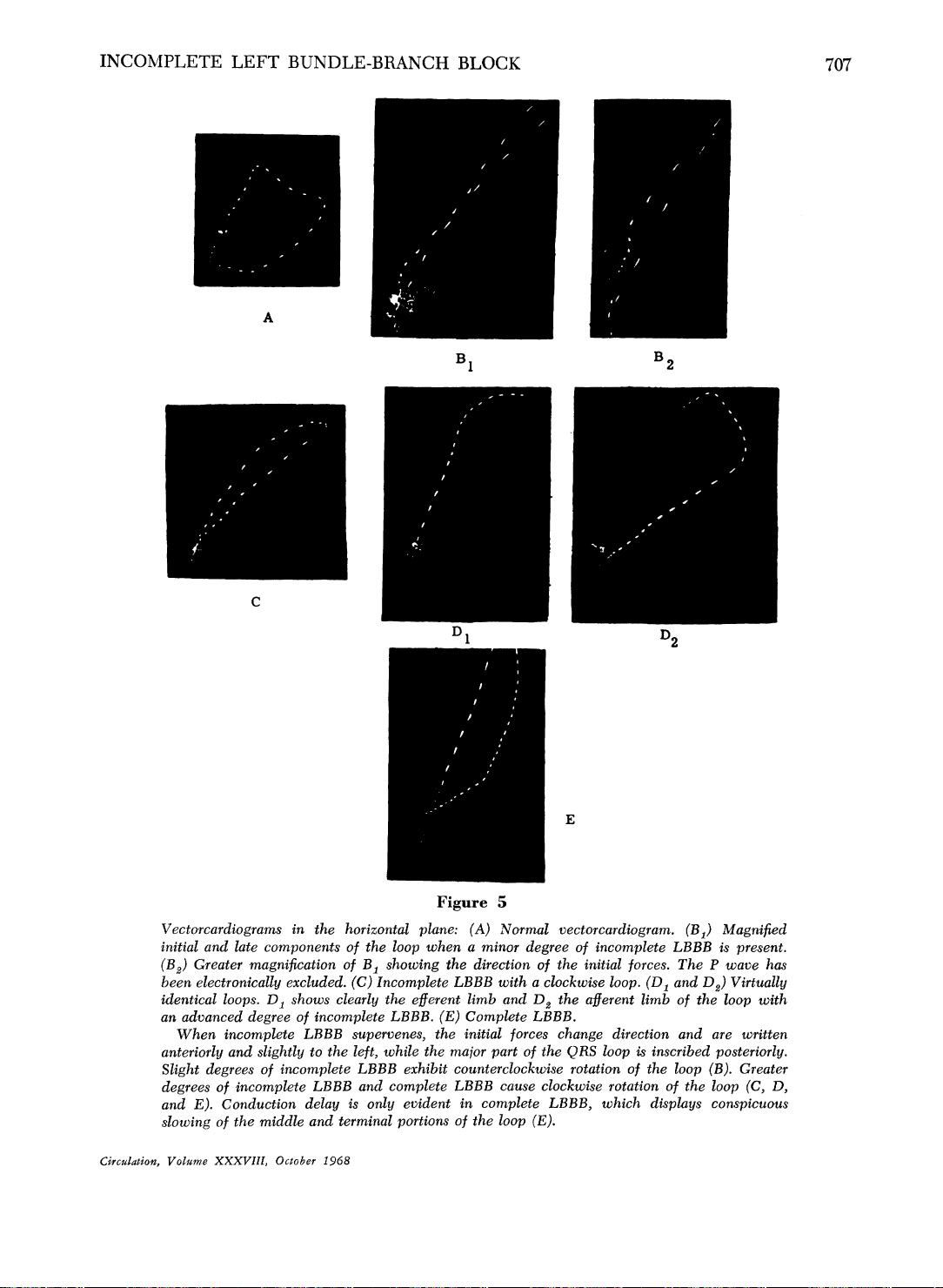
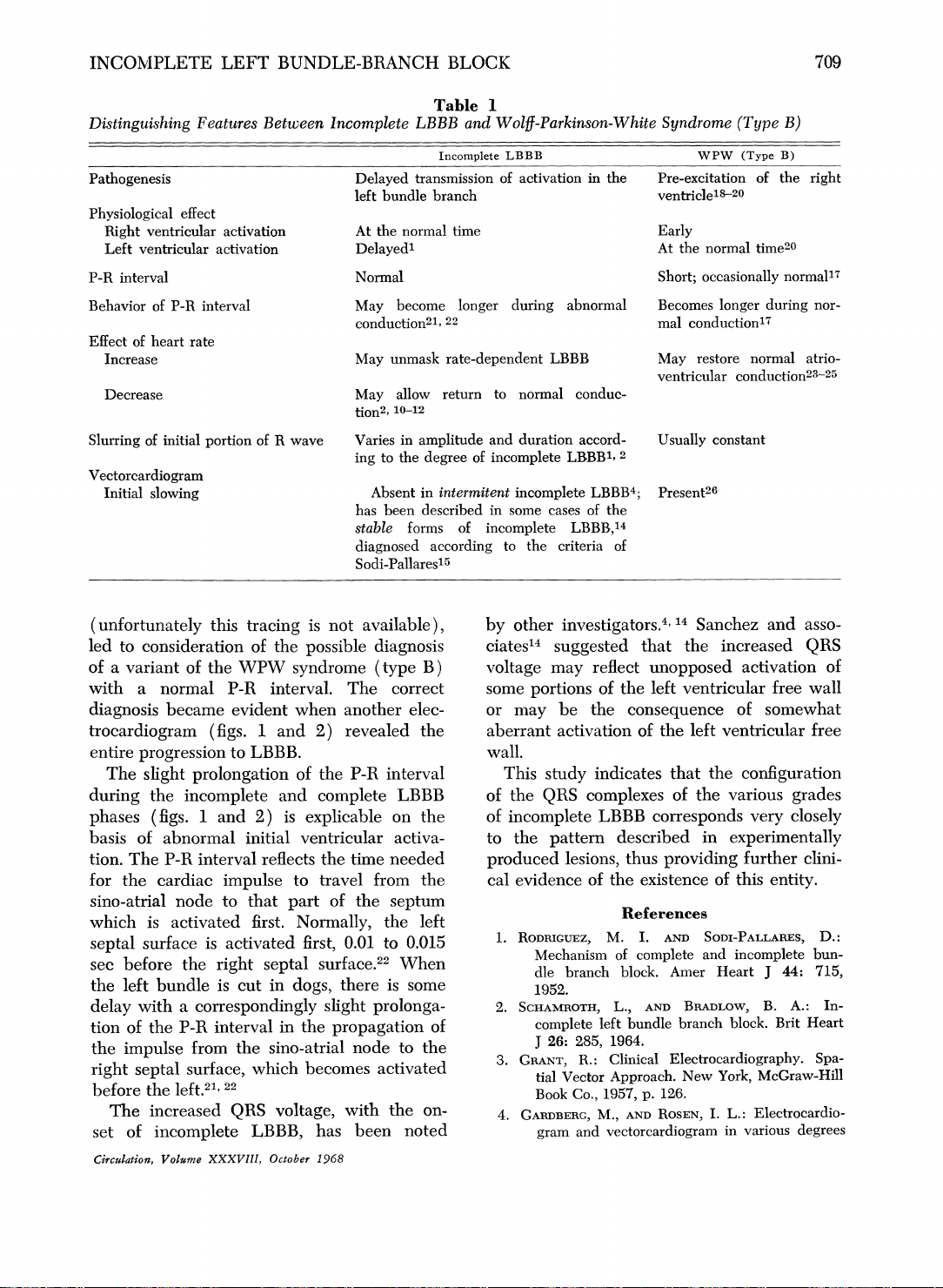
Incomplete Left Bundle-Branch Block: A Definite Electrocardiographic Entity
Incomplete Left Bundle-Branch Block: A Definite Electrocardiographic Entity. Tài liệu được sưu tầm giúp bạn tham khảo, ôn tập và đạt kết quả cao. Mời bạn đọc đón xem.
Môn: Tài liệu Tổng hợp 3.6 K tài liệu
Trường: Tài liệu khác 3.9 K tài liệu
Tác giả:

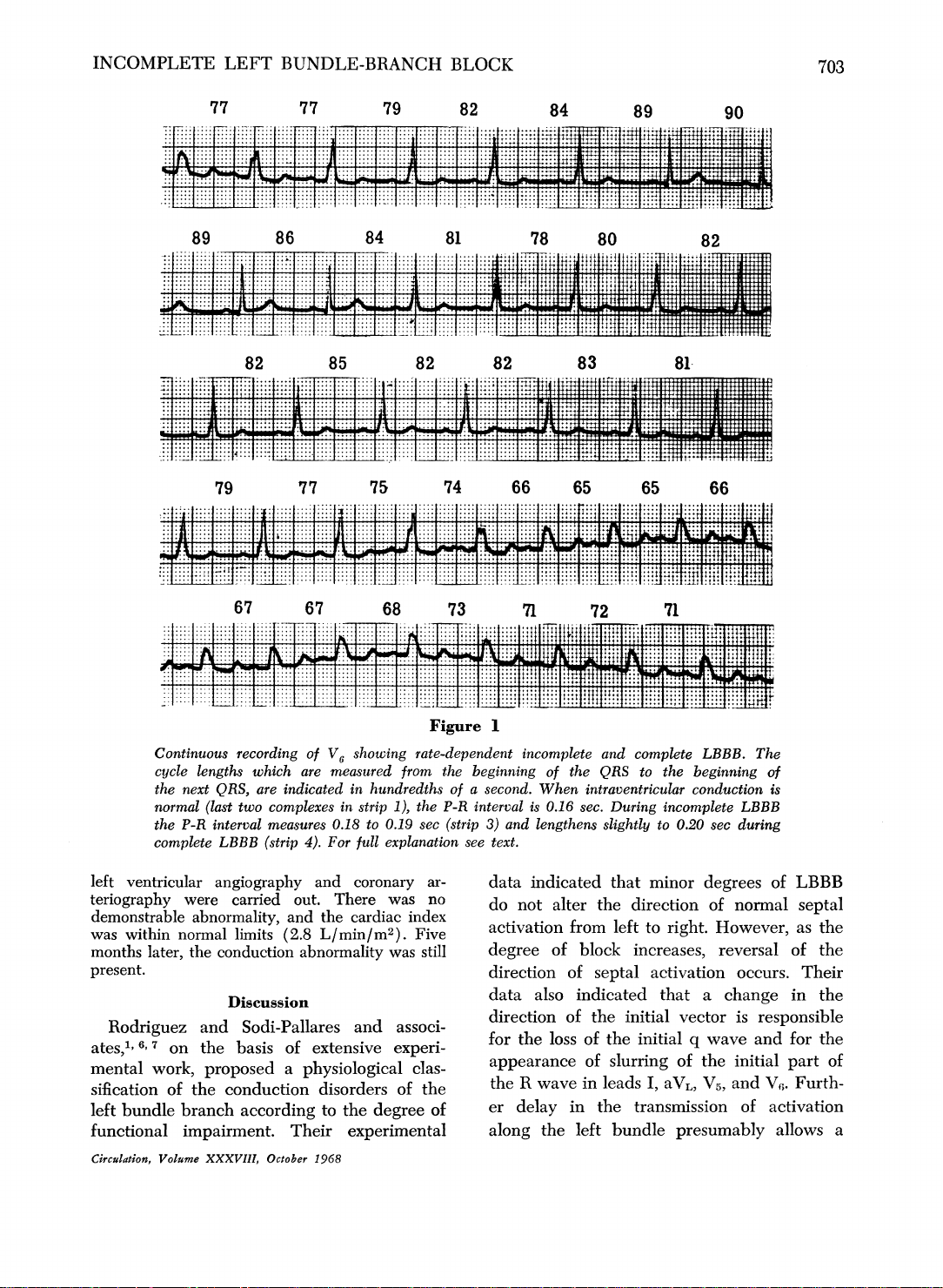
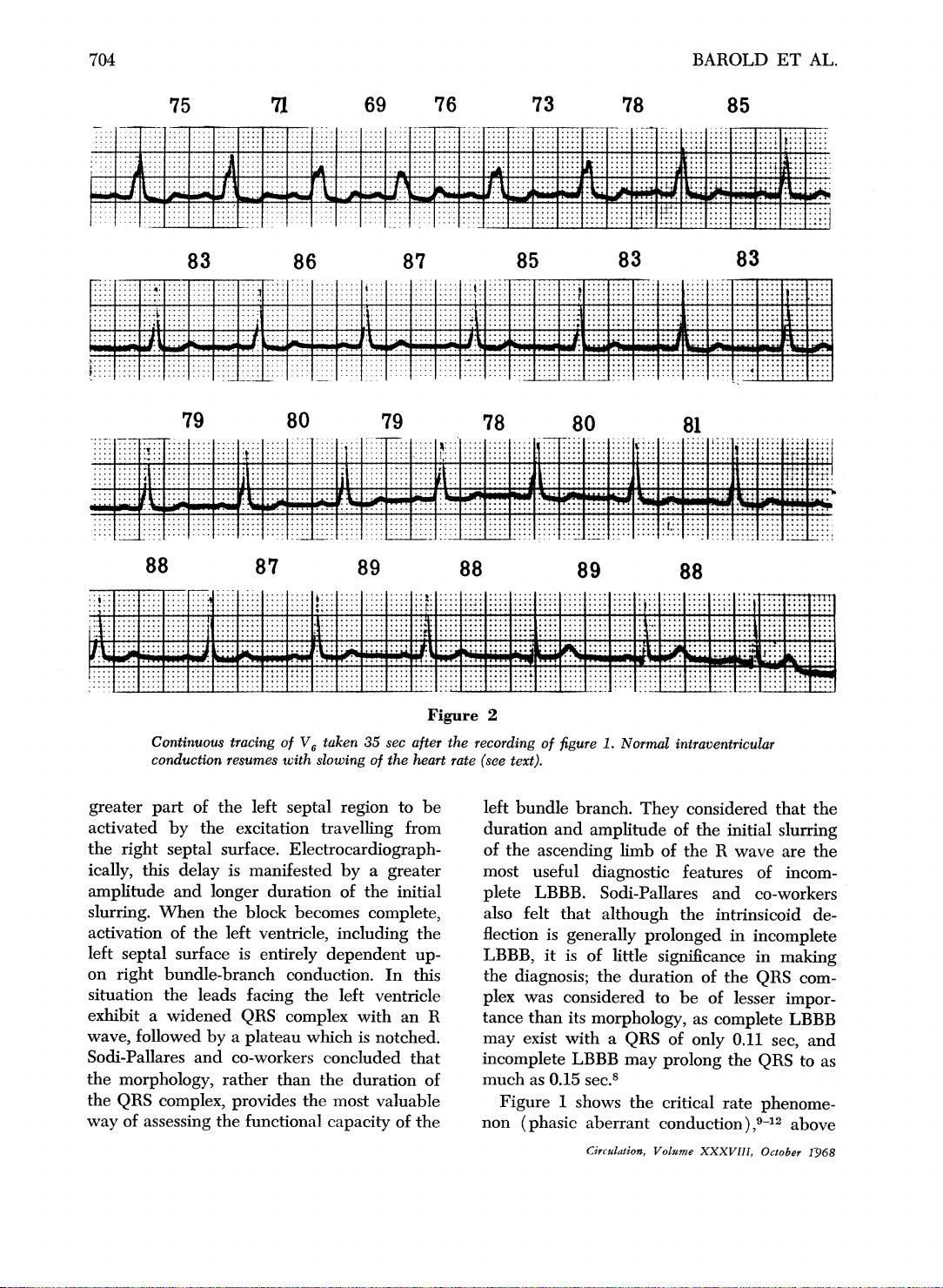
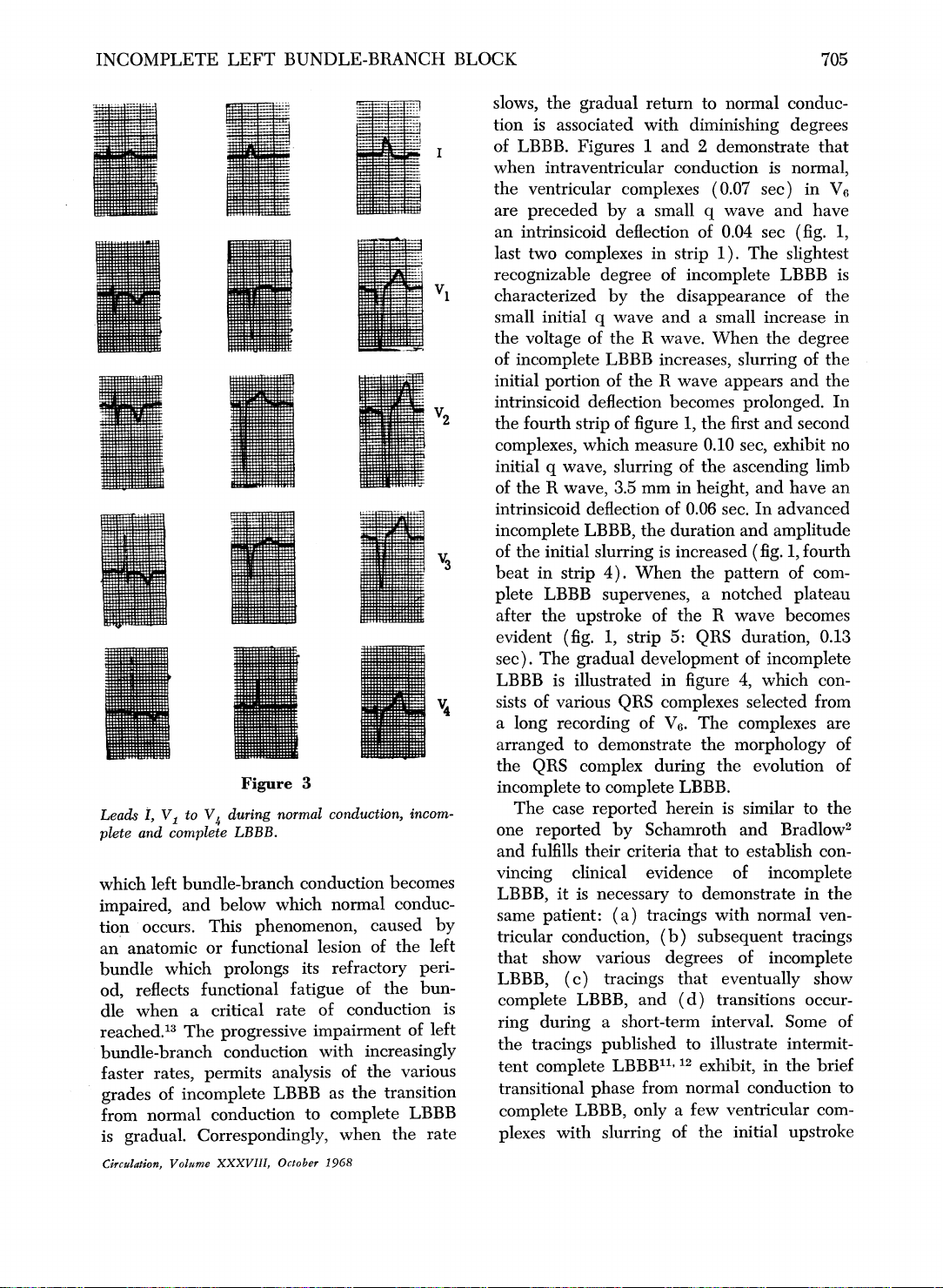
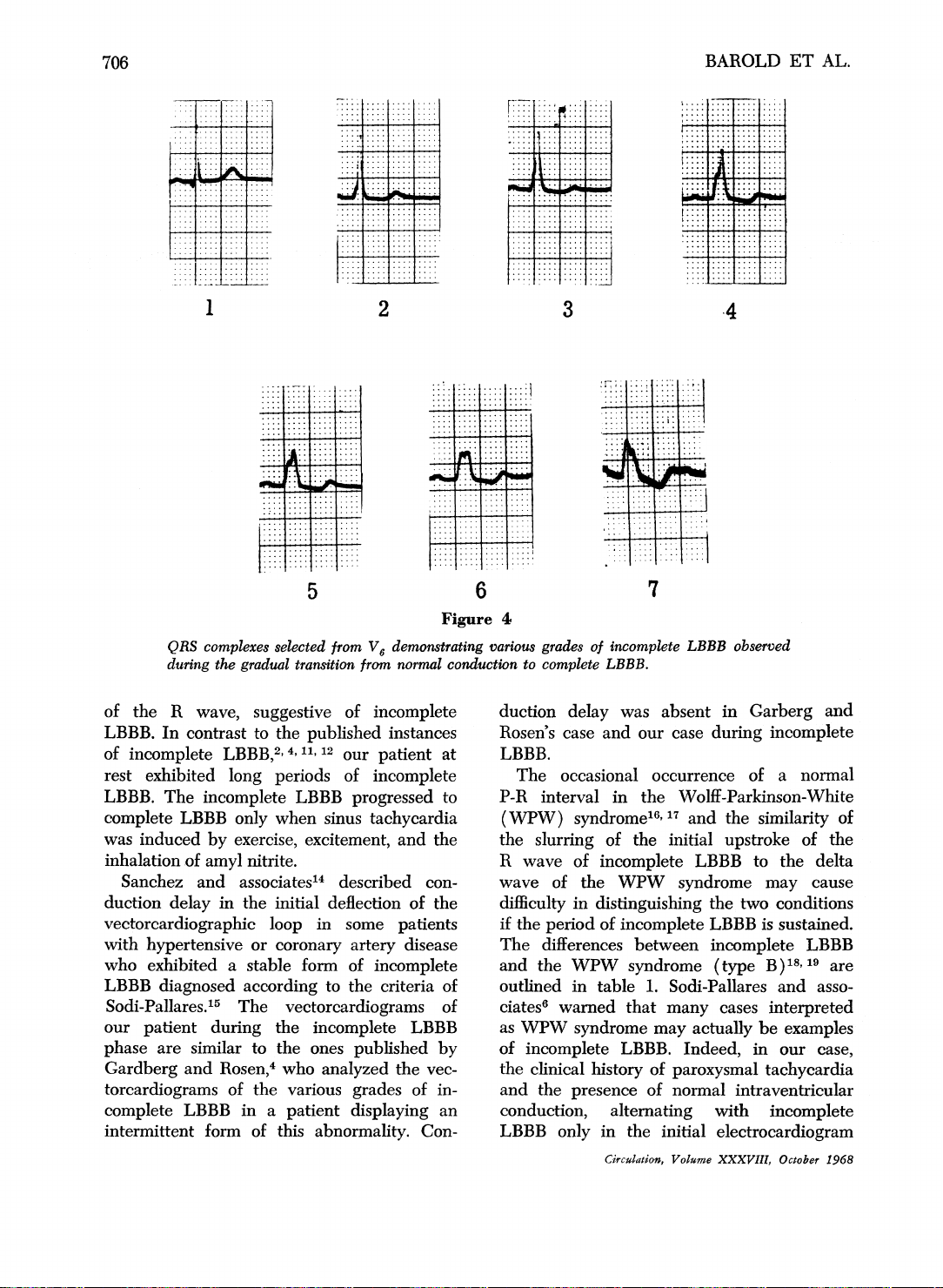


Preview text:
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Downloaded from http://ahajournals.org by on May 20, 2025
Tài liệu liên quan:
-
Ung dung game hoa trong cac chien dich MKT
18 9 -
Bao cao Chi so TMDT Viet Nam 2025
15 8 -
Thông tư quy định về việc phân quyền, phân cấp và phân định thẩm quyền quản lý nhà nước về giáo dục cho chính quyền địa phương
23 12 -

Nghị quyết về phát huy các giá trị di sản văn hóa gắn với phát triên du lịch bền vững tỉnh Khánh Hòa đến năm 2025, định hướng đến năm 2030
13 7 -

Quyết định phê duyệt Chiến lược phát triển du lịch Việt Nam đến năm 2030
13 7