No hay diferencias pre 6 y 24 hrs - tài liệu tham khảo | Đại học Hoa Sen
No hay diferencias pre 6 y 24 hrs - tài liệu tham khảo | Đại học Hoa Sen và thông tin bổ ích giúp sinh viên tham khảo, ôn luyện và phục vụ nhu cầu học tập của mình cụ thể là có định hướng, ôn tập, nắm vững kiến thức môn học và làm bài tốt trong những bài kiểm tra, bài tiểu luận, bài tập kết thúc học phần, từ đó học tập tốt và có kết quả cao cũng như có thể vận dụng tốt những kiến thức
Môn: Corporate Finance (CF2033) 92 tài liệu
Trường: Trường Đại học Hoa Sen 5.3 K tài liệu
Tác giả:




Preview text:
Article ID: WMC001717 ISSN 2046-1690
Characterization of the Effects of One Maximal
Repetition Test on Muscle Injury and Inflammation Markers Corresponding Author: Dr. Sandro M Hirabara,
Professor, ICAFE, Cruzeiro do Sul University, Rua Galvão Bueno, 868, 01506-000 - Brazil Submitting Author: Dr. Sandro M Hirabara,
Professor, ICAFE, Cruzeiro do Sul University, Rua Galvão Bueno, 868, 01506-000 - Brazil Article ID: WMC001717
Article Type: Research articles
Submitted on:09-Mar-2011, 07:04:41 PM GMT Published on: 10-Mar-2011, 09:56:03 PM GMT
Article URL: http://www.webmedcentral.com/article_view/1717
Subject Categories:PHYSIOLOGY
Keywords:One Repetition Maximum Test, Muscle Damage, Inflammation, Creatine Kinase, C-Reactive Protein,
How to cite the article:Barquilha G , Uchida M C, Santos V C, Moura N R, Lambertucci R H, Hatanaka E ,
Cury-Boaventura M F, Pithon-Curi T C, Gorjão R , Hirabara S M. Characterization of the Effects of One Maximal
Repetition Test on Muscle Injury and Inflammation Markers . WebmedCentral PHYSIOLOGY 2011;2(3):WMC001717 Source(s) of Funding:
This work was supported by CNPq, FAPESP and CAPES. Competing Interests:
This study has no competing interests.
WebmedCentral > Research articles Page 1 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM
Characterization of the Effects of One Maximal
Repetition Test on Muscle Injury and Inflammation Markers
Author(s): Barquilha G , Uchida M C, Santos V C, Moura N R, Lambertucci R H, Hatanaka E , Cury-Boaventura
M F, Pithon-Curi T C, Gorjão R , Hirabara S M Abstract
been poorly studied. Here, we evaluated the effects of
1 RM on muscle injury and inflammatory markers in healthy subjects.
We assessed the influence of the one repetition
Resistance exercise has been shown to be an
maximum (1RM) bench press exercise on the
important intervention for promoting and maintaining
temporal profile of markers of muscular injury (creatine
health and quality of life. However, the physiological
kinase - CK - activity) and inflammation (interleukin-2 -
changes promoted by resistance exercise are under
IL-2, IL-1 , tumoral necrose factor-a - TNF- , IL-6, and
investigation yet. It is noteworthy to date that no
C-reactive protein - CRP). Participants were 11
studies are found about the muscle damage and
healthy subjects both genders (eight men and three
inflammation caused by the 1RM test in healthy
women), active, involved in strength training, for subjects.
recreational purposes for more than six months.
Analysis of markers of muscular injury and
Characteristics of the volunteers were: age (21.5 ± 6.5
inflammation is frequently used to investigate whether
years), weight (70.1 ± 21.1 kg), height (172.8 ± 52.1
there is muscle damage induced by exercise (Glesson
cm), and fat mass (14.5 ± 5.7 %). Sample blood was
2002; Margonis et al. 2007; Uchida et al. 2009). The
colleted before the 1 RM test and at 1 h, 24 h, 48 h,
activity of the creatine kinase (CK) in blood has been
and 6 days after the test. Statistical analysis was
used as a main surrogate marker of muscle damage,
performed using ANOVA with repeated measurements
resulting from eccentric exercise (Stupka et al. 2000;
and Bonferroni post-test. There was a significant
Totsuka et al. 2002; Evans et al. 2002; Nosaka et al.
increase in the CK activity after 6 days of the test
2002a; Nosaka et al. 2002b; Tartibian et al. 2009). The
when compared to pre-test time, whereas CRP activity
increase CK activity in plasma indicates that there was
increased 24 and 48 hours when compared to pre-test
a release of the enzyme due to a rupture of the muscle
period. There was not significant difference in the
cell membrane (muscle damage), considering that CK
plasma cytokine levels. Although 1 RM test did not
does not have the ability to cross the membrane when
alter the levels of inflammatory cytokines, it can be
the sarcoplasm is intact (Brown et al. 1997;
observed through this work that this test can induce
Brancaccio et al. 2007). Increased plasma activity of
muscle damage, which would be a negative factor for
this enzyme is influenced by both the volume and
athletes, since the muscle injury and inflammation are
intensity of exercise (Tiidus and Ianuzzo 1983; Uchida
associated with decreased performance, especially et al. 2009). strength and muscle power.
Tissue damage leads to activation of the immune Introduction
defense cells, the leukocytes, in order to remove
unwanted elements arising from such injury (Pyne
1994). When activated, the leukocytes can stimulate
the release of proinflammatory cytokines such as
Before the prescription of resistance exercise, it is
tumor necrosis factor- (TNF- ) and interleukins (IL),
common to use some tests in order to evaluate muscle
IL-8 and IL-6. These factors stimulate the release of
strength and track, as for example the one repetition
anti-inflammatory cytokines as IL-1ra and may also
maximum test (1 RM test). This test, by raising the
stimulate the acute phase proteins, such as C-reactive
maximum weight possible in a single complete
protein (CRP) (Nieman et al. 2005; Smith 2000b;
movement, aims to stimulate the dynamic maximum
Robson 2003; Steensberg et al. 2003).
strength by the practitioner (Ware et al. 1995). The 1
RM test has several advantages, such as low cost,
Abrupt increases in markers of muscle damage and
easy implementation, specificity, and ability to adapt to
inflammation resulting from intense muscle effort can
reality of various sports (Barnard et al. 1999). However,
affect the immune system and metabolism, impairing
physiological changes induced by the 1 RM test have
the performance of athletes (Nieman 2007;
WebmedCentral > Research articles Page 2 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM
Steensberg et al. 2003). The 1 RM test is greatly and
mesuarements, followed by the Tukey post-test, was
frequently used for measuring muscle strength, but its
performed to verify the statistical differences. Criterion
effects on muscle damage and inflammatory process
for statistical significance was set at p <0.05.
is not known yet. Thus, the purpose of this study was Results
to assess the influence of the 1RM bench press
exercise on the temporal profile of markers of
muscular injury and inflammation in healthy subjects.
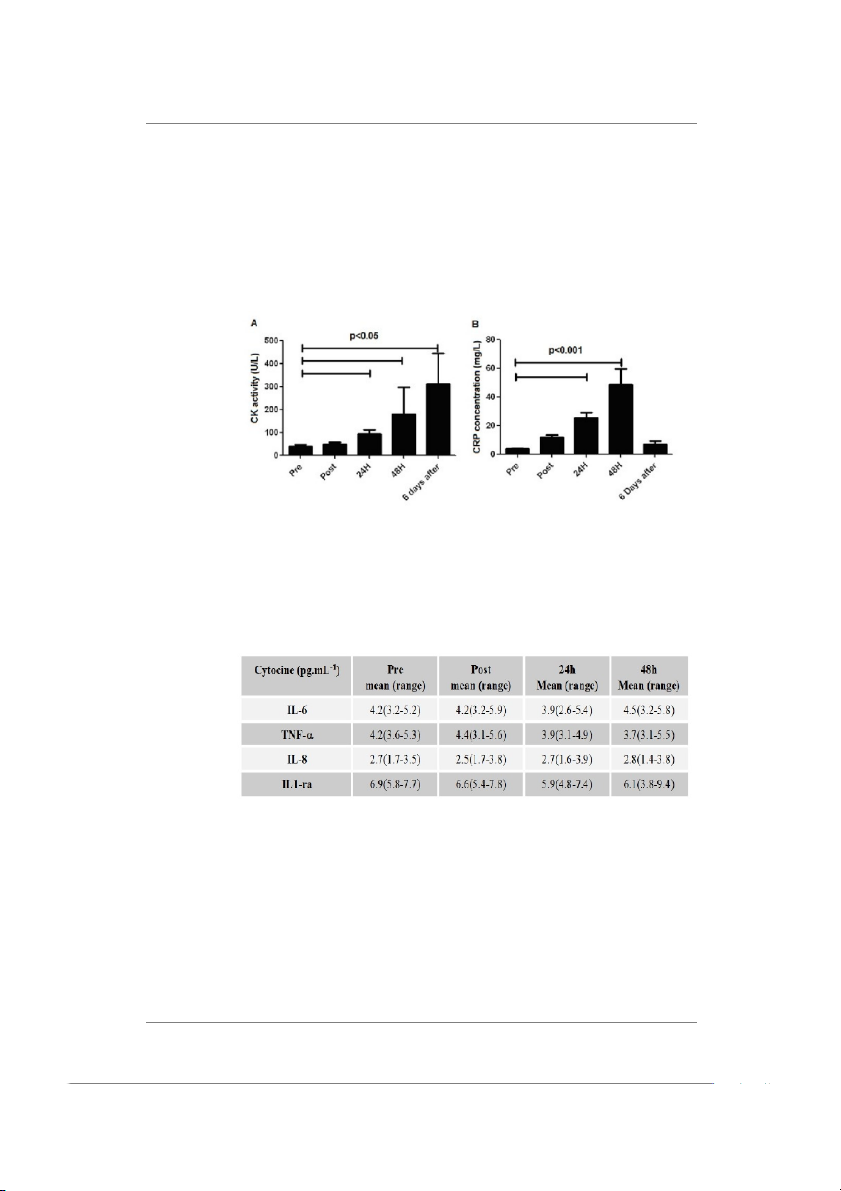
Illustration 1 shows the activity of CK and the Methods
concentration of CRP in plasma (Illustration 1A and 1B,
respectively). The 1 RM test increased the CK activity
after 24 h, remaining elevated up to 6 days after the Subjects
test (p<0.05) in a time-dependent manner (Ilustration
Participants of the study were 11 healthy subjects both
1A). CRP concentration was elevated 24 h after the 1
genders (eight men and three women), active,
RM test (p<0.001), remained elevated up to 48 h
involved in strength training, for recreational purposes
(p<0.001) and returned to the basal value at 6 days
for more than six months. Characteristics of the
after the test (Illustration 1B). No changes in the
volunteers were: age (21.5 ± 6.5 years), weight (70.1
pro-inflammatory cytokines IL-6, TNF-a, IL-8 and
± 21.1 kg), height (172.8 ± 52.1 cm), and fat mass
IL-1Ra induced by 1 RM test were found (Illustration
(14.5 ± 5.7 %). The subjects voluntarily signed a 2).
consent form. This study was approved by the ethics Discussion
committee and research of the Cruzeiro do Sul
University (protocol No. 039/2009).
Exercise protocol (1 RM test)
Although a growing number of studies focusing the
For the determination of 1 RM in a bench press
changes in markers of inflammation and injury during
exercise, participants were instructed to grip the bar at
and after resistance exercise, nothing is known about
a comfortable position, which was typically 10 to 20
the physiological aspect of the test after completion of
cm wider than shoulder width (Kim et al. 2002).
a 1 RM test, one exercise of high intensity and low
Subjects performed a warm-up consisting in 3 sets: 1st
volume. In this study, we found a linear increase in
set: 8–10 repetitions using a light weight (~ 50% of 1
activity of CK at the times 24 h, 48 h, and 6 days after
RM); 2nd set: 3–5 repetitions using a moderate weight
the 1 RM test. Studies have shown that CK may
(~ 70% 1 of RM); 3rd set: 1–3 repetitions using a heavy
remain increased up to 7 days after the execution of
weight (~ 80% of 1RM). After the warm-up, each
an effort (Brancaccio et al. 2007; Bruunsgaard et al.
participant was submitted to the 1 RM test by 1997).
increasing the resistance on subsequent attempts until
Uchida et al. (2009) conducted a study which aimed to
he or she was unable to finalize a full correct
investigate muscle damage in different intensities in
movement. Approximately 5 sets of one repetition
bench press exercise. The intensities were 50%, 75%,
were accomplished and each attempt was separated
90% and 110% of 1 RM. The activity of CK enzyme
by 3 min of rest (Shimano et al. 2006). The 1 RM tests
increased significantly in all groups after bout, with no
were accomplished by two trained spotters.
significant difference among groups, probably because
Determination of the CK, plasma interleukin
the total volumes were similar among them. Already
concentrations and serum CRP
Paschalis and colleagues (Paschalis et al. 2005)
compared two different protocols of resistance
CK activity and CRP were determined by a highly
exercise, with a moderate and one with high intensity,
sensitive immunoturbidimetric method (Bioclin
finding a significant increase of CK in both protocols.
Diagnostics, São Paulo, Brazil), according to the
But, it is noteworthy that the highest value of CK
manufacturer’s instructions. Plasma concentrations of
IL-6, IL-8, TNF- , and IL-1ra were determined based
activity presented in this study was found in the group
who performed intense exercise, showing that the
on the enzyme-linked immunosorbent assay (ELISA),
intensity of exercise is the major factor in modulating
using a Duoset Kit (Quantikine, R&D Systems, the response of CK activity.
Minneapolis, MM, USA), following the manufacturer’s instructions.
Were also evaluated some markers of muscle
inflammation. These markers were cytokines (IL-8, Statistical analysis
IL1R-a, TNF- and IL-6), which did not show
Analysis of variance (ANOVA) with repeated
significant changes with the test of 1RM. Our results
WebmedCentral > Research articles Page 3 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM
corroborate the findings of Uchida et al. (2009) and
test of high intensity and low volume can lead to
Hirose et al. (2004), who also found no significant
induction of muscle damage, which would be a
changes of the cytokines analyzed with a protocol of
negative factor for the athletes, since the muscle injury
strength training. The Ushida’study (2009) evaluated
and inflammation are associated with decreased
the cytokines IL-6 and IL-1 , in addition to TNF- . No
performance, especially strength and muscle power.
significant change was found in none of these
Therefore, special care must be taken in introducing
cytokines in any of intensities studied (50, 75, 90 and
the 1RM test in sports periodization.
110% of 1 RM). Hirose et al. (2004) investigated the Abbreviation(s)
effect of a protocol of eccentric exercise (6 sets of 5
repetitions in exercise of elbow flexors) in several
cytokines, among them the IL-1ra, IL-6, IL-8 and TNF-
. These cytokines, in corroborating with our results,
1 RM, one repetition maximum; IL, interleucin; TNF,
were not significantly modified by the eccentric
tumoral necrosis factor; CK, creatine kinase; CRP,
exercise. Changes in plasma cytokines have been C-reactive protein
found in exercises cyclic bulk (Toft et al. 2000; Nieman Acknowledgement(s)
2001). Thus, one possible reason for the lack of
alteration of cytokines in our study is the small volume
used by the 1 RM test. In addition, an important factor
that should be taken into account is the difficulty in
This study was supported by grants from FAPESP,
detecting cytokines in plasma, due to the short time CNPq, and CAPES.
that they are stable (Petersen and Pedersen 2005). References
In the present study, we found an increase in acute
phase protein CRP, which peaked at 48 hours after te
1 RM test. CRP has proinflammatory characteristics
1. Barnard KL, Adams KJ, Swank AM, Mann E, Denny
(activation of the complement system and
DM (1999) Injuries and muscle soreness during the
opsonization of bacteria) and anti-inflammatory (to
one repetition maximum assessment in a cardiac
prevent the adhesion of neutrophils to endothelial cells,
rehabilitation population. Journal of Cardiopulmonary
inhibit the generation of superoxide by neutrophils and Rehabilitation 19:52-58.
stimulating the synthesis of the receptor antagonist
2. Brancaccio P, Maffulli N, Limongelli FM (2007)
IL-1) (du Closs 2000; Epstein 1999, Semple et al.
Creatine kinase monitoring in sport medicine. British
2004). Taylor et al. (1987) found an increase of 300%, Medical Bulletin 81:209-230.
24 hours after performing a triathlon race. Semple and
3. Brown SJ, Child SH, Donnelly AE (1997)
colleagues (2004) also found a significant increase of
Exercise-induced skeletal muscle damage and
this protein after an ultramarathon. It is well known that
aaptations following repeated bouts of eccentric
the cytokines IL-6 and TNF- stimulate the production
muscle contractions. Journal of Sports Sciences
of acute-phase proteins, such as CRP (Semple et al. 15:215-222.
2004; Du Closs 2000). In our study we found a
4. Bruunsgaard H, Galbo H, Halkjaer-Kristensen J,
significant increase in CRP, but was not detected
Johansen TL, MacLean DA, Pedersen BK (1997)
increased IL-6 and TNF- , possibly because the CRP
Exercise-induced increase in serum interleukin-6 in
is more stable in plasma than cytokines, which are
humans is related to muscle damage. Journal of
more difficult to detect (Pedersen 2005). Physiology 15:833–841.
In conclusion, the 1 RM test (a session of high
5. Clarkson PM, Hubal MJ (2002) Exercise-induce
intensity, but low volume) was enough to increase CK
Muscle Damage in Humans. American Journal of
activity and CRP concentration in the plasma. These
Physiology Rehabilitation 81:52-69.
results suggest that indeed there were muscle
6. Du Clos TW (2000) Function of C-reactive protein.
damage and inflammatory response (increased CRP) Annals of Medicine 32:274-278.
after the 1 RM test. Concentration of pro-inflammatory
7. Evans RK, Knight KL, Draper DO, Parcell, AC (2002)
cytokines, however, was not modified by the test.
Effects of warm-up before eccentric exercise on
indirect markers of muscle damage. Medicine and Conclusion(s)
Science & Sports and Exercise 34:1892–1899.
8. Epstein FH (1999) Acute phase proteins and other
systemic responses to inflammation. The New
The 1RM test is widely used by athletes of various
England Journal of Medicine 340:448-454.
sports. It can be observed through this work that this
WebmedCentral > Research articles Page 4 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM
9. Fallon KE (2001) The acute phase response and
during exercise. Sports Medicine 17:245-258.
exercise: The ultra-marathon as prototype exercise.
23. Robson PJ (2003) Elucidating the unexplained
Clinical Journal of Sports Medicine 11:38-43.
underperformance syndrome in endurance athletes:
10. Gleeson M (2002) Biochemical and immunological
the interleukin-6 hypothesis. Sports Medicine
markers of overtraining. Journal of Sports Science and 33:771-778. Medicine 1:31-41
24. Semple SJ, Smith LL, McKune AJ, Neveling N,
11. Hirose L, Nosaka K, Newton M, Laveder A, Kano
Wadee A (2004) alterations in acute-phase reactants
M, Peake J, Suzuki K (2004) Changes in inflammatory
(CRP, rheumatoid factor, complement, factor B, and
mediators following eccentric exercise of the elbow
immune complexes) following an ultramarathon. South
flexors. Exercise Immunology Reviews 10:75-1090.
African Journal of Sports Medicine 20:17-21.
12. Kim PS, Mayhew JL, Peterson DF (2002). A
25. Shimano T, Kraemer WJ, Spiering BA, Volek JS,
modified YMCA bench press test as a predictor of 1
Hatfield DL, Silvestre R, Vingren JL, Fragala MS,
repetition maximum bench press strength. Journal of
Maresh CM, Fleck SJ, Newton RU, Spreuwenberg LP,
Strength and Conditioning Research 16:440–445.
Hakkinen K (2006). Relationship between the number
13. Lake MJ, Lafortune MA (1998) Mechanical inputs
of repetitions and selected percentages of one
related to perception of lower extremity impact loading
repetition maximum in free weight exercises in trained
severity. Medicine and Science & Sports and Exercise
and untrained men. Journal of Strength and 30:136-143
Conditioning Research 20:819–823.
14. Margonis K, Fatouros IG, Jamurtas AZ, Nikolaidis
26. Smith LL, Anwar A, Fragen M, Rananto C, Holbert
MG, Douroudos I, Chatzinikolaou A, Mitrakou A,
D (2000a) Cytokines and cell adhesion molecules
Mastorakos G, Papassotiriou I, Taxildaris K, Kouretas
associated with high-intensity eccentric exercise.
D (2007) Oxidative stress biomarkers responses to
European Journal of Applied Physiology 82:61-67.
physical overtraining: Implications for diagnosis. Free
27. Smith LL (2000b) Cytokine hypothesis of
Radical Biology and Medicine 43:901-910.
overtraining: a physiological adaptation to excessive
15. Nieman DC, Davis JM, Henson DA, Gross SJ,
stress? Medicine and Science & Sports and Exercise
Dumke CL, Utter AC, Vinci DM, Carson JA, Brown A, 32:317-331.
McAnulty LS, Triplett NT (2005) Muscle cytokine
28. Steensberg A, Fischer CP, Keller C, Møller K,
mRNA changes after 2.5 h of cycling: influence of
Pedersen BK (2003) IL-6 enhances plasma IL-1ra,
carbohydrate. Medicine and Science & Sports and
IL-10, and cortisol in humans. American Journal Exercise 37:1283-1290.
Physiology Endocrinology Metabolism 285:433-437.
16. Nieman DC (2007) Marathon training and immune
29. Stupka N, Lowther S, Chorneyko K, Bourgeois JM,
function. Sports Medicine 37:412-415.
Hogben C, Tarnopolsky MA (2000) Gender differences
17. Nieman DC, Dru A, Henson LL, Smith AC, Utter
in muscle inflammation after eccentric exercise.
DM, Vinci J, Mark D, David E, Shute M (2001)
Journal of Applied Physiology 89:2325-2332.
Cytokine changes after a marathon race. Journal of
30. Taylor C, Rogers G, Goodman C, Baynes RD,
Applied Physiology 91:109–114.
Bothwell TH, Bezwoda WR, Kramer F, hattingh J
18. Nosaka K, Newton M, Sacco P (2002a).
(1987) Hematologic, iron-lelated, and acute-phase
Delayed-onset muscle soreness does not reflect the
protein responses to sustained strenuous exercise.
magnitude of eccentric exercise-induced muscle
Journal of Applied Physiology 62:464-469.
damage. Scandinavian Journal of Medicine and
31. Tartibian B, Azadpoor N, Abbasi, A (2009) Effects
Science in Sports 12:337–346.
of two different type of treadmill running on human
19. Nosaka K, Newton M, Sacco, P. (2002b). Muscle
blood leukocyte populations and inflammatory indices
damage and soreness after endurance exercise of the
in young untrained men. Journal of Sports Medicine
elbow flexors. Medicine and Science in Sports and
and Physical Fitness 49:214-223. Exercise 34:920–927.
32. Tiidus PM, Ianuzzo CD (1983) Effects of intensity
20. Paschalis V, Koutedakis Y, Jamurtas AZ, Mougios
and duration of muscular exercise on delayed
V, Baltzopoulos V (2005) Equal volumes of high and
soreness and serum enzyme activities. Medicine and
low intensity of eccentric exercise in relation to muscle
Science & Sports and Exercise 15:461-5.
damage and performance. Journal of Strength and
33. Totsuka M, Nakaji S, Suzuki K (2002) Break point
Conditioning Research 19:184–188.
of serum creatine kinase release after endurance
21. Petersen AM, Pedersen BK (2005) The
exercise. Journal of Applied Physiology 93:1280-1286.
anti-inflammatory effect of exercise. Journal of Applied
34. Toft AD, Thorn M, Ostrowski K, Asp K, Møller K, Physiology 98:1154–1162
Iversen S et al. N-3 polyunsaturated fatty acids do not
22. Pyne DB (1994) Regulation of neutropil function
affect cytokine response to strenuous exercise.
WebmedCentral > Research articles Page 5 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM
Journal of Applied Physiology 89:2401–2406.
35. Uchida MC, Nosaka K, Ugrinowitsch C, Yamashita
A, Martins JE, Moriscot AS, Aoki MS (2009) Effect of
bench press exercise intensity on muscle soreness
and inflammatory mediators. Journal of Sports Sciences 27:499-507.
36. Ware JS, Clemens CT, Mayhew JL, Johnston TJ
(1995) Muscular endurance repetitions to predict
bench press and squat strength in college football
players. Journal of Strength and Conditioning Research 9:99-103.
WebmedCentral > Research articles Page 6 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM Illustrations Illustration 1
??Means and standard deviations of the activity of CK (A) and concentration of CRP (B) at
baseline (pre) and after the 1RM test session at 1 h (post), 24 h, 48 h, and 6 days. Illustration 2
Mean (and range) of the concentrations of L-6, IL-8, IL-1ra and TNF-a at baseline (pre) and
after the 1 RM test session at 1 h, (post), 24 h, and 48 h.
WebmedCentral > Research articles Page 7 of 8 WMC001717
Downloaded from http://www.webmedcentral.com on 07-Sep-2011, 11:54:03 AM Disclaimer
This article has been downloaded from WebmedCentral. With our unique author driven post publication peer
review, contents posted on this web portal do not undergo any prepublication peer or editorial review. It is
completely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscript
but also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions before
submitting any information that requires obtaining a consent or approval from a third party. Authors should also
ensure not to submit any information which they do not have the copyright of or of which they have transferred
the copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater to
the needs of an individual patient. The web portal or any content(s) therein is neither designed to support, nor
replace, the relationship that exists between a patient/site visitor and his/her physician. Your use of the
WebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harm
that you may suffer or inflict on a third person by following the contents of this website.
WebmedCentral > Research articles Page 8 of 8
Tài liệu liên quan:
-

Lý do chọn đề tài báo cáo trong công việc - Tài liệu tham khảo | Đại học Hoa Sen
466 233 -

Models for warehouse management Classification and Project - Tài liệu tham khảo | Đại học Hoa Sen
222 111 -

Project Report Room for rent Group 4 - Tài liệu tham khảo | Đại học Hoa Sen
306 153 -

Brealey Fo CF 8ed Chapter 5 - Tài liệu tham khảo | Đại học Hoa Sen
291 146 -

Top 200 câu hỏi trắc nghiệm phân tích đầu tư và chứng khoán - Tài liệu tham khảo | Đại học Hoa Sen
1 K 482